

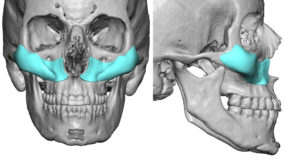
The placement of facial implants has a major influence on their aesthetic outcome, particularly that of symmetry. Temporal, cheek and jaw angle implants are particularly prone to postoperative asymmetries because they usually paired or bilateral placements. While the placement of bilateral facial implants may seem uncomplicated and straightforward to do, the reality is that they are two independent operations where the placement of one implant is completely separate from its opposite side.
Cheek implants are the most frequently done bilateral facial implant augmentation procedure. Using standard implant styles and sizes, I would say that asymmetric cheek implant placement is the norm…as seen in many 3D CT scan images. It is very rare to actually see perfect or close to perfect cheek implant placements. Fortunately the thickness of the overlying soft tissues dampens the implant asymmetry so it is always less severe aesthetically than how the implant placements appears on 3D CT images.
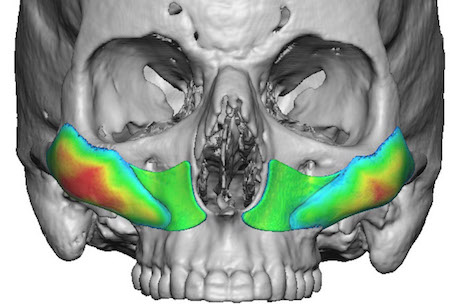
In custom cheek implants the need for symmetric placement is magnified as they are often bigger in terms of surface area coverage. As a result more minor amounts of implant asymmetry produce greater amounts of external aesthetic asymmetry. It is typical to build into the implant design orientation markers for positioning and I have used a variety of techniques to do so.
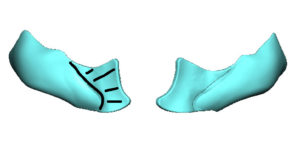
 One technique that I have found to be most successful for custom cheek implant placement is a maxillary orientation ‘tab’ that can be cut away once placed. It covers most of the face of the maxilla, is 2mms thick and has a line between it and the cheek implant itself. This larger orientation tab provides multiple reference points (infraorbital nerve, bony edge of the pyriform aperture, tooth roots) to orient it in place. Because the cheek implant is attached to it, if the orientation tab is correctly placed then the cheek implant must be also.
One technique that I have found to be most successful for custom cheek implant placement is a maxillary orientation ‘tab’ that can be cut away once placed. It covers most of the face of the maxilla, is 2mms thick and has a line between it and the cheek implant itself. This larger orientation tab provides multiple reference points (infraorbital nerve, bony edge of the pyriform aperture, tooth roots) to orient it in place. Because the cheek implant is attached to it, if the orientation tab is correctly placed then the cheek implant must be also.
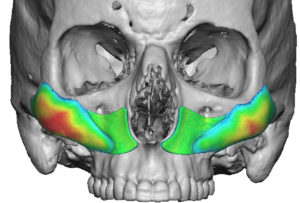
An interesting observation on the placement of cheek implants, which is most commonly done through an intraoral approach, is that the back end of the implant can never be seen. The point of incisional access is furtherest away from the implant’s posterior zygomatic bone location and curves down away from a direct line of sight. (not to mention the front edge of the implant blocks what is happening behind it) As a result orientation of the implant is best done but what can be seen…the anterior surface of the maxilla.
Dr. Barry Eppley
Indianapolis, Indiana