


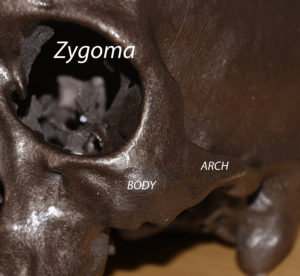
Cheekbone reduction surgery is a well known double osteotomy technique for narrowing the width of the face. It uses an anterior zygomatic body bone cut combined with a release of the back end of the zygomatic arch from the temporal bone process. This then allows the cheekbone bone segment to be moved inward making the cheekbones more narrow.
While these two cheekbone osteotomy cuts are often thought of as always being done together, that is not necessarily so. The anterior cheekbone osteotomy can be done in isolation for cheek widening and is known as the zygomatic sandwich osteotomy. (ZSO) It gets this name because a graft or implant is placed between the osteotomy cut line like a sandwich to create the widening effect.
 T
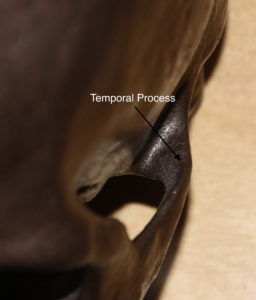
T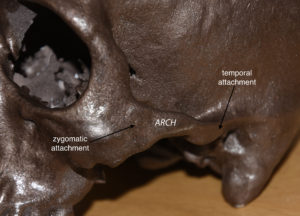 he posterior zygomatic arch osteotomy can also be done in isolation which is far less well known. It is done to create a narrowing effect back closer to the ear. To understand how it works it is helpful to appreciate the anatomy of the posterior zygomatic arch as it joins with the temporal bone through its temporal process. This often can be the widest part of the entire zygomatic arch and can stick out further than the rest of the cheekbone.
he posterior zygomatic arch osteotomy can also be done in isolation which is far less well known. It is done to create a narrowing effect back closer to the ear. To understand how it works it is helpful to appreciate the anatomy of the posterior zygomatic arch as it joins with the temporal bone through its temporal process. This often can be the widest part of the entire zygomatic arch and can stick out further than the rest of the cheekbone.
 To make this posterior cheekbone area more narrow and create a smoother transition from the temples across the zygomatic arch into the lower face, an isolated posterior zygomatic arch osteotomy can be done. This effect can be seen in an anatomic illustration showing the location of the osteotomy cut at the very end of the zygomatic arch.
To make this posterior cheekbone area more narrow and create a smoother transition from the temples across the zygomatic arch into the lower face, an isolated posterior zygomatic arch osteotomy can be done. This effect can be seen in an anatomic illustration showing the location of the osteotomy cut at the very end of the zygomatic arch.

 The posterior zygomatic arch osteotomy (PZO) is done through a 10mm vertical incision at the backside of the sideburn in men or the preauricular hair tuft in women. This provides direct access to the planned osteotomy site. The osteotomy is done at the most posterior point on the arch where it joins the zygomatic process of then temporal bone. An angled bone cut is done with a reciprocating saw and the anterior segment moved inward with an osteotome. The remaining intact zygomatic process of the temporal bone is then burred down for a complete reduction of the prominence. A small 1.5mm three-hole step plate is then applied with 1.5 x 4mm long self-drilling screws.
The posterior zygomatic arch osteotomy (PZO) is done through a 10mm vertical incision at the backside of the sideburn in men or the preauricular hair tuft in women. This provides direct access to the planned osteotomy site. The osteotomy is done at the most posterior point on the arch where it joins the zygomatic process of then temporal bone. An angled bone cut is done with a reciprocating saw and the anterior segment moved inward with an osteotome. The remaining intact zygomatic process of the temporal bone is then burred down for a complete reduction of the prominence. A small 1.5mm three-hole step plate is then applied with 1.5 x 4mm long self-drilling screws.
The PZO is useful as a stand alone procedure or as a secondary procedure when it remains still protrusive after a prior cheekbone reduction procedure. The effect of moving in the tail of the zygomatic. arch is enhanced if the zygomatfuc process of the temporal bone is concurrently reduced.
Dr. Barry Eppley
Indianapolis, Indiana