

Festoons are a unique midface aesthetic issue with an anatomic complex basis that occurs in the prezygomatic space. Loss of fat volume of the subcutaneous fat and laxity of the orbicularis retaining ligament, SOOF and overlying skin are major elements in their formation. As a result they appear as hammocks or bags of loose tissue that hang down. In contrast fluid accumulation in this area are malar mound which are frequently confused with that of festoons.
Festoon are a difficult aesthetic midface issue that has a high recurrence rate with many treatment approaches. The traditional lower blepharoplasty approach with subperiosteal dissections, various methods of releases and large skin excisions initially appear to be effective but recurrence rates are high. This is not to say that many patients do not get improvement, it is just not as profound or sustained as that seen at the end of these procedures.
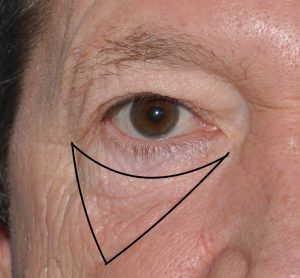 In the November 2023 issue of the journal Plastic and Reconstructive Surgery an article on this topic was published entitled ‘Mini-incision Direct Festoon Access, Cauterization, and Excision (MIDFACE): A 12-Year Analysis of a Novel Festoon Surgery’. In this paper the authors review their over a decade experience in 75 patients with a festoon surgical approach. In this technique an upside down triangle is initially drawn with three vertices. A lateral limb (1 cm lateral to the lateral canthus to the bottom of the outer festoon edge), a medial limb (1 cm below the medial canthus along the inferior edge of the festoon – ZCL line) and finally a scalloped line between the medial and lateral cantonal points – OML like) This triangle marked the territory of the festoon. A 1 cm incision is then marked a preseptal orbicularis line. Subciliary lower eyelid incisions are made and a skin flap (preorbicularis) is raised down to the infraorbital rim. Subcutaneous fat at the lateral limb of the festoon is reduced by electrocautery. A button hole incision through the muscle is made to remove any herniated orbital fat. An external skin incision is made along the marked perceptual line and dissected under the body of the festoon to the level of the SOOF. The SOOF is then grasped and pulled upward toward the incision and cauterized. This SOOF cauterization is done in a circumferential manner to shrink the festoon. Once completed any excess skin and oribicularus muscle can be removed and a two layer closure done with 6-0 plain. A limited amount of lower eyelid skin is removed and the subciliary incision closed. No specific anchoring or suspensions of the skin flap are done.
In the November 2023 issue of the journal Plastic and Reconstructive Surgery an article on this topic was published entitled ‘Mini-incision Direct Festoon Access, Cauterization, and Excision (MIDFACE): A 12-Year Analysis of a Novel Festoon Surgery’. In this paper the authors review their over a decade experience in 75 patients with a festoon surgical approach. In this technique an upside down triangle is initially drawn with three vertices. A lateral limb (1 cm lateral to the lateral canthus to the bottom of the outer festoon edge), a medial limb (1 cm below the medial canthus along the inferior edge of the festoon – ZCL line) and finally a scalloped line between the medial and lateral cantonal points – OML like) This triangle marked the territory of the festoon. A 1 cm incision is then marked a preseptal orbicularis line. Subciliary lower eyelid incisions are made and a skin flap (preorbicularis) is raised down to the infraorbital rim. Subcutaneous fat at the lateral limb of the festoon is reduced by electrocautery. A button hole incision through the muscle is made to remove any herniated orbital fat. An external skin incision is made along the marked perceptual line and dissected under the body of the festoon to the level of the SOOF. The SOOF is then grasped and pulled upward toward the incision and cauterized. This SOOF cauterization is done in a circumferential manner to shrink the festoon. Once completed any excess skin and oribicularus muscle can be removed and a two layer closure done with 6-0 plain. A limited amount of lower eyelid skin is removed and the subciliary incision closed. No specific anchoring or suspensions of the skin flap are done.
Their results showed no significant complications in the 75 treated patients. Photographic analysis of 39 patients showed sustained improvement in the festoons, no incision show and high patient satisfaction. Patient assessment for why these festoons occurred included by their history genetics, prior injections treatment (e.g., fillers), previous facial surgery, alcohol, and sun exposure.
In this MIDFACE technique for festoon correction they have shown a high success rate for a procedure that is relatively minimal invasive by comparison to other techniques. The success of the procedure is attributed to a more direct access to the SOOF where suture and heat-induced fibrosis create the effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon