

Craniotomies that involve the frontal and/or frontotemporal bones are commonly done for a variety of intracranial problems such as bleeding from trauma or for access to tumors. While the bone flap is put back into position using low profile plates and screws and the detached temporalis muscle resuspended, residual skull deformities are common.
Frontal skull deformities can occur if the bone flap settles to any degree as it heals or the craniotomy line does not heal by bony union. This can leave a palpable edge or visible ridge across the forehead along the original craniotomy line. A portion of the forehead may also be flatter or more recessed. The temporal region can also develop a visible concavity due to temporalis muscle atrophy from its initial detachment.
 These after craniotomy contour defects of the forehead and temple region can be built back up by bone cement augmentation very successfully. But it is not always necessary to completely reopen part or all of the original scalp incision. This incision (now scar) is often way far back from the forehead region and may be well healed with regrowth of hair around it. A more direct and simpler approach to the forehead defects can be done through a pretrichial or hairline approach. Bone cement can be introduced through this closer and more limited incisional access.
These after craniotomy contour defects of the forehead and temple region can be built back up by bone cement augmentation very successfully. But it is not always necessary to completely reopen part or all of the original scalp incision. This incision (now scar) is often way far back from the forehead region and may be well healed with regrowth of hair around it. A more direct and simpler approach to the forehead defects can be done through a pretrichial or hairline approach. Bone cement can be introduced through this closer and more limited incisional access.
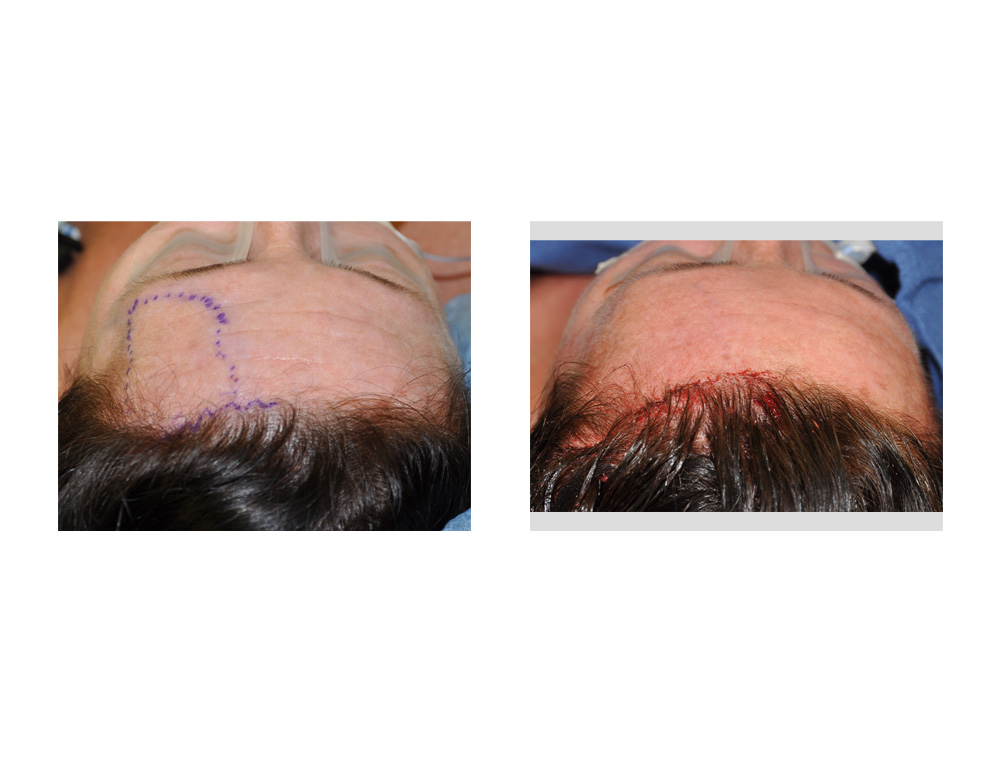
The pretrichial incision is a standard approach for a cosmetic browlift so it usually heals in an inconspicuous manner. Using an irregular or zigzag incision pattern that parallels the frontal hairline ensures that it will heal with a scar that is hidden along its edge. The pretrichial approach to craniotomy defects of the forehead in selected patients can simplify the secondary correction of their residual contour problems.
Dr. Barry Eppley
Indianapolis, Indiana