

While the entire face can be affected by congenital asymmetry the lower jaw is commonly involved. Beyond the severe congenital jaw asymmetries which are associated with major brachial arch deficiencies (e.g., hemifacial microsomia) the far more common jaw asymmetries are more ‘aesthetic’ in nature. This means that the occlusion is fine and there may not even be much of an occlusal cant but there are moderate changes in the shape of the jaw. Depending upon the type of facial asymmetry the lower jaw can be vertically short and pulled up with an overall vertical facial shortening. The other type of lower jaw asymmetry is when it is vertically longer due to an overgrowth on that side and that side of the face is longer.
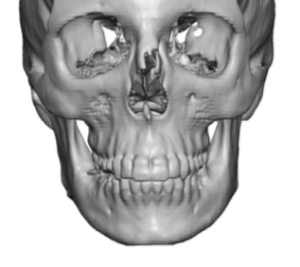
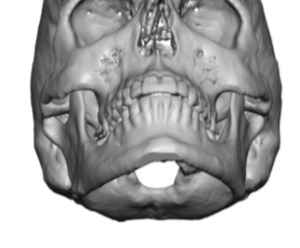
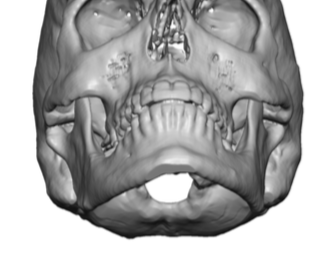
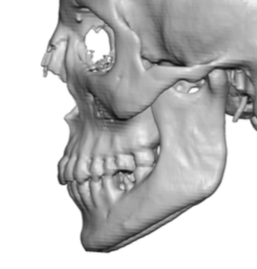 In the lower or vertically longer type of lower jaw asymmetry there is a discrepancy in the levels of the inferior borders between the two sides. These asymmetries can be a few millimeters or more and are easily seen in 3D CT scans or even a simple panorex x-ray. The complete differences in the levlel of the inferior borders can be appreciated by looking. at the side view in the 3D CT scan from the good or desired side. That will show the exact difference in both its vertical or horizontal extent and represents the ideal amount to remove.
In the lower or vertically longer type of lower jaw asymmetry there is a discrepancy in the levels of the inferior borders between the two sides. These asymmetries can be a few millimeters or more and are easily seen in 3D CT scans or even a simple panorex x-ray. The complete differences in the levlel of the inferior borders can be appreciated by looking. at the side view in the 3D CT scan from the good or desired side. That will show the exact difference in both its vertical or horizontal extent and represents the ideal amount to remove.
 In removing an elongated inferior border of the lower jaw there are two approaches, submental and intraoral. The submental approach provides linear access from the chin which is ideal when using a sagittal reciprocating saw to do the bone removal. It stays way below the mental nerve so potential lower lip numbness is not a potential complication. It is limited by how far back one can go which will stop short of affecting any jaw angle bone removal. It also results in a small submental scar to perform it but this is not usually a major issue for most patients.
In removing an elongated inferior border of the lower jaw there are two approaches, submental and intraoral. The submental approach provides linear access from the chin which is ideal when using a sagittal reciprocating saw to do the bone removal. It stays way below the mental nerve so potential lower lip numbness is not a potential complication. It is limited by how far back one can go which will stop short of affecting any jaw angle bone removal. It also results in a small submental scar to perform it but this is not usually a major issue for most patients.

 From the submental incision it is necessary to create subperiosteal tissue elevation on the side as well as the inferior border onto the inner surface. Using a reciprocating saw a measured full thickness bone cut can be made with the saw as far back as it will reach. The longest saw blade is used. The bone cut stops just short of going all the way through the inner surface of the bone and the cut is completed by small osteotomies. The bone segment is then removed. With a good cut at the right level a single bone segment removal completes the vertical asymmetry correction or as much correction as is possible.
From the submental incision it is necessary to create subperiosteal tissue elevation on the side as well as the inferior border onto the inner surface. Using a reciprocating saw a measured full thickness bone cut can be made with the saw as far back as it will reach. The longest saw blade is used. The bone cut stops just short of going all the way through the inner surface of the bone and the cut is completed by small osteotomies. The bone segment is then removed. With a good cut at the right level a single bone segment removal completes the vertical asymmetry correction or as much correction as is possible.
Dr. Barry Eppley
Indianapolis, Indiana