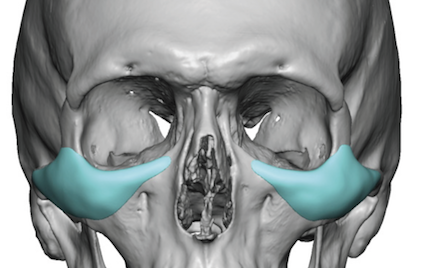


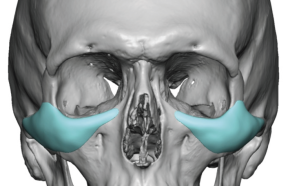
 The midface equivalent of the custom jawline implant of the lower face is the custom infraorbital-malar (IOM) implant. Besides the break for the nose this is an implant that augments the convexity of the midface from under the eye out onto the zygomatic body and arch. While it is possible in some smaller IOM implants to place them through the mouth this is almost never a good idea as that incisional access is the furtherest removed from the location of the implant. It also comes at the horizontal implantation site in a vertical direction which increases the risk of implant malposition not to mention a higher infection risk by the intraoral approach.
The midface equivalent of the custom jawline implant of the lower face is the custom infraorbital-malar (IOM) implant. Besides the break for the nose this is an implant that augments the convexity of the midface from under the eye out onto the zygomatic body and arch. While it is possible in some smaller IOM implants to place them through the mouth this is almost never a good idea as that incisional access is the furtherest removed from the location of the implant. It also comes at the horizontal implantation site in a vertical direction which increases the risk of implant malposition not to mention a higher infection risk by the intraoral approach.
 The best incisional approach for most IOM implants is through the lower eyelid. This allows direct vision onto the entire orbital rim for the dissection and implant placement as well provides linear access for the zygomatic arch dissection. While the lower eyelid carries its own risks it is actually less traumatic than intraoral placement, has a a more assured implant placement, and a lower risk of infection.
The best incisional approach for most IOM implants is through the lower eyelid. This allows direct vision onto the entire orbital rim for the dissection and implant placement as well provides linear access for the zygomatic arch dissection. While the lower eyelid carries its own risks it is actually less traumatic than intraoral placement, has a a more assured implant placement, and a lower risk of infection.
 But it is important to understand that the lower blepharoplasty incision for IOM implants is different than how it is done for the more typical rejuvenative lower eyelid procedure. First it does not cross the entire lower eyelid. It is more of a hemi-lid incision that only needs to be made on the lateral half of the lower eyelid with a very small lateral canthal extension of a few millimeters. By not crossing over the whole lower eyelid a significant amount of the orbicularis muscle is preserved. When this is combined with the lack of any tissue removal, as occurs in the typical excisional lower blepharoplasty, the risk of ectropion and lower eyelid malposition is significantly decreased. Since many IOM implants raise the height of the infraorbital rim as well as add structure to the cheeks, support for the lower eyelid position is increased.
But it is important to understand that the lower blepharoplasty incision for IOM implants is different than how it is done for the more typical rejuvenative lower eyelid procedure. First it does not cross the entire lower eyelid. It is more of a hemi-lid incision that only needs to be made on the lateral half of the lower eyelid with a very small lateral canthal extension of a few millimeters. By not crossing over the whole lower eyelid a significant amount of the orbicularis muscle is preserved. When this is combined with the lack of any tissue removal, as occurs in the typical excisional lower blepharoplasty, the risk of ectropion and lower eyelid malposition is significantly decreased. Since many IOM implants raise the height of the infraorbital rim as well as add structure to the cheeks, support for the lower eyelid position is increased.
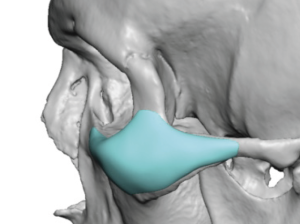
 After a skin-muscle flap is raised and the bony infraorbital rim identified the complete subperiosteal dissection is done with electrocautery release from the nasal bone across the rim and out onto the front end of the zygomatic arch. Once the zygomatic arch is reached blind subperiosteal dissection is done guided externally by palpation of the arch bone. Dissection is done past the maximal convexity of the arch onto its downward slope towards the ear. It is also important to get down over the zygomatic body into the submalar space. The implant is then inserted by placing the outer half in first and then folding the infraorbital rim segment into the more narrow medial pocket. Once in proper position it is secured with a single 1.6mm self-tapping screw.
After a skin-muscle flap is raised and the bony infraorbital rim identified the complete subperiosteal dissection is done with electrocautery release from the nasal bone across the rim and out onto the front end of the zygomatic arch. Once the zygomatic arch is reached blind subperiosteal dissection is done guided externally by palpation of the arch bone. Dissection is done past the maximal convexity of the arch onto its downward slope towards the ear. It is also important to get down over the zygomatic body into the submalar space. The implant is then inserted by placing the outer half in first and then folding the infraorbital rim segment into the more narrow medial pocket. Once in proper position it is secured with a single 1.6mm self-tapping screw.
The lower eyelid incision is closed with cheek tissue and lateral orbicularis muscle resuspension and 6-0 plain sutures for the skin. This is an incision that heals extremely well, being inconspicuous in most patients. It offers the bets access for most assured implant placement with the lowest risk of infection.
Dr. Barry Eppley
Indianapolis, Indiana