

While most patients understandably are enamored with the design and surface area coverage of a custom jawline implant, one aspect of it that is not obvious is its placement during surgery. How can such a large implant be placed through small incisions that heal well and create no obvious aesthetic tradeoffs?
One approach that diminishes the scar risk is that two out of three incisions used in custom jawline implants are intraoral. For the creation of the posterior jawline dissection and pocket, paired (bilateral) vestibular incisions are used opposite the 2nd and 3rd molars. (if present) The only external skin incision used, particularly in men, is a submental one underneath the chin. In women with smaller implants an intraoral incision behind the lower lip may be used.
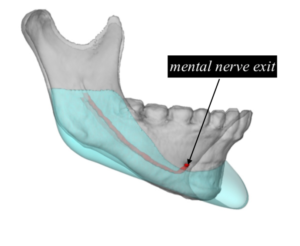 In many jawline implants they may be able to be placed from introducing the implant through the anterior approach. In passing the implant from front to back the most important issue is not to injure the mental nerve which lies at the superior end of the narrowest part of the pocket. (between the chin and the jaw angles) This nerve comes out of the bone and supplies feeling to the lower lip and anterior teeth. Getting the highest part of the implant (jaw angles) under the mental nerve is the challenge in doing so.
In many jawline implants they may be able to be placed from introducing the implant through the anterior approach. In passing the implant from front to back the most important issue is not to injure the mental nerve which lies at the superior end of the narrowest part of the pocket. (between the chin and the jaw angles) This nerve comes out of the bone and supplies feeling to the lower lip and anterior teeth. Getting the highest part of the implant (jaw angles) under the mental nerve is the challenge in doing so.
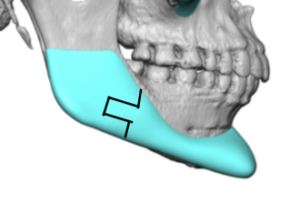 One very useful technique in jawline implants to protect the mental nerve is to section it into several pieces. I had done so for years using a midline split technique through the chin (two piece geometric split) and passing the implant in two calfs from back to front. But when the chin part of the implant is very large the midline split technique still poses a risk of nerve injury. An alternative strategy is the three piece geometric split back at the front end of the jaw angles. In this approach the chin part is put in through the submental incision while the jaw angle part is put in through the intraoral incisions.
One very useful technique in jawline implants to protect the mental nerve is to section it into several pieces. I had done so for years using a midline split technique through the chin (two piece geometric split) and passing the implant in two calfs from back to front. But when the chin part of the implant is very large the midline split technique still poses a risk of nerve injury. An alternative strategy is the three piece geometric split back at the front end of the jaw angles. In this approach the chin part is put in through the submental incision while the jaw angle part is put in through the intraoral incisions.

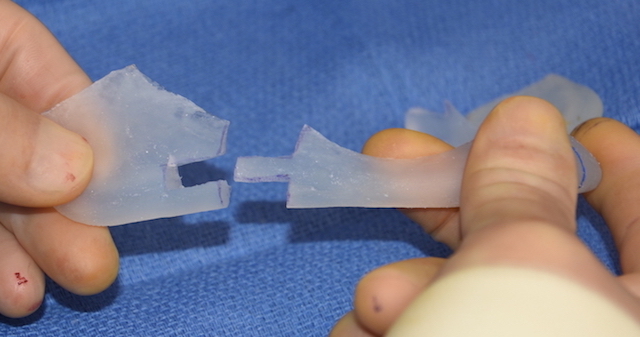
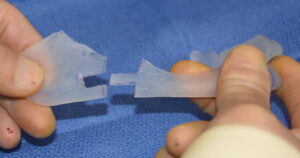 The slotted design allows the jaw angles on both sides to be snapped back together. This protects the mental nerve because the largest parts of the implant, the chin and jaw angles, does not need to be passed under the mental nerve.
The slotted design allows the jaw angles on both sides to be snapped back together. This protects the mental nerve because the largest parts of the implant, the chin and jaw angles, does not need to be passed under the mental nerve.
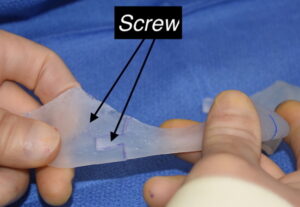
 Once reassembled back together inside the pocket, two screws are placed in a percutaneous fashion to securely hold their position together.
Once reassembled back together inside the pocket, two screws are placed in a percutaneous fashion to securely hold their position together.
While solid silicone offers flexibility of a large implant like that of the custom jawline implant, it is still stiff enough that innovative placement strategies are still needed.
Dr. Barry Eppley
Indianapolis, Indiana