

The term ‘jaw reduction’ has evolved over the years to mean different types of procedures. Originally jaw reduction referred to an orthognathic surgery operation where the lower jaw was set back by an either a vertical oblique or sagittal split osteotomy to correct a malocclusion. It could also have referred to an aesthetic procedure of a reducing the front part of the jaw. (chin) More rarely it may have referred to a partial excision of the masseter muscle.
While jaws reduction may still refer to these long standing procedures its meaning has taken a different flavor being currently influenced by one of the more popular lower facial reshaping procedures in the world…V-line surgery. V-line surgery is the ultimate jaw reduction procedure as it reduces the size of the lower jaw from the jaw angles to the chin. While starting in Asian populations such as China and South Korea to reduce the ethnic tendencies for large jaw developments it is now widely applied to facial feminization efforts in non-Asians as well.
 Traditional V-line surgery is a partial jaw amputation procedure in which the shape of the posterior jaw angles and jawline is vertically removed at an angle up to the chin. The chin is then reduced/narrowed usually through a t-shaped genioplasty tis complete the jaw reduction. While a tremendously effective procedure in terms pf achieving a lower jaw reduction it is important to remember that theV-line surgery was developed on patients who had naturally larger jaw structures. By the intraoral method by which the procedure is done there is no such thing as a limited or just a little bit of jaw reduction. The procedure is an ‘all in’ proposition which is why in some patients who have more normal size jaws they end up with too much jaw bone removal and develop ‘V-line surgery regret’. (and may even want to partially or fully restore the lost jawline)
Traditional V-line surgery is a partial jaw amputation procedure in which the shape of the posterior jaw angles and jawline is vertically removed at an angle up to the chin. The chin is then reduced/narrowed usually through a t-shaped genioplasty tis complete the jaw reduction. While a tremendously effective procedure in terms pf achieving a lower jaw reduction it is important to remember that theV-line surgery was developed on patients who had naturally larger jaw structures. By the intraoral method by which the procedure is done there is no such thing as a limited or just a little bit of jaw reduction. The procedure is an ‘all in’ proposition which is why in some patients who have more normal size jaws they end up with too much jaw bone removal and develop ‘V-line surgery regret’. (and may even want to partially or fully restore the lost jawline)
Regardless of who V-line surgery is done on the one well known adverse sequelae of jaw bone removal is loose skin.When you reduce bony support by stripping off soft tissue attachments there is going to be more lax skin. The only question is how significant will the issue be and will the patient want some form of a jowl tuck procedure.
As a result it is important to recognize that traditional V-line surgery is not for everyone. A modification of traditional V-line is what I call the Western version. Rather than reducing jaw size by changing its shape jaw width can be reduced by thinning the bone but leaving its vertical shape intact. While this can be done by generalized burring I prefer the corticotomy technique which creates more predictable bone removal and is also faster to perform.
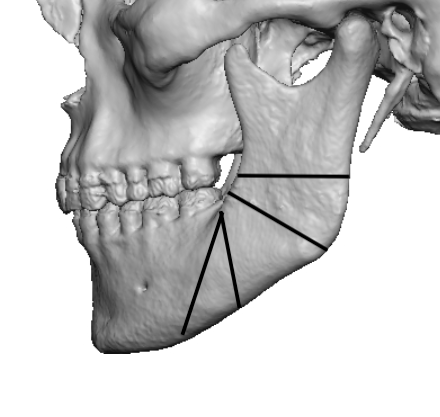
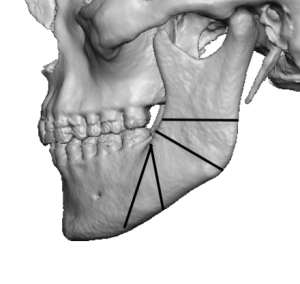 In the outer corticotomy technique bone cuts are made through the outer cortex of the angle and body of the jaw using a reciprocating saw. These bone cuts are made in a radiating pattern from the ascending ramus incision site. The outer cortex is known to both exist and be able to be removed based on sagittal split ramus osteotomies. This is also a known site and method for harvesting cortical bone grafts.
In the outer corticotomy technique bone cuts are made through the outer cortex of the angle and body of the jaw using a reciprocating saw. These bone cuts are made in a radiating pattern from the ascending ramus incision site. The outer cortex is known to both exist and be able to be removed based on sagittal split ramus osteotomies. This is also a known site and method for harvesting cortical bone grafts.

 Once these bone cuts are complete an osteotome (chisel) is used to carefully chip off the outer cortical bone between the corticotomy cuts. This will expose the very thin marrow space between the two cortical layers of the ramus. The marrow space is much bigger as one transitions between the angle and the body of the lower jaw. From that area forward the outer cortex can be reduced by burring. The chin can then be reduced if needed by various chin reduction procedures including t-shaped genioplasties.
Once these bone cuts are complete an osteotome (chisel) is used to carefully chip off the outer cortical bone between the corticotomy cuts. This will expose the very thin marrow space between the two cortical layers of the ramus. The marrow space is much bigger as one transitions between the angle and the body of the lower jaw. From that area forward the outer cortex can be reduced by burring. The chin can then be reduced if needed by various chin reduction procedures including t-shaped genioplasties.
Traditional V-line surgery is best utilized when the jaws angles are of medium to long lengths and/or when one wants to avoid any risk of soft tissue sagging.. But in high jaw angle patients width reduction is what is needed and the shape of the jaw angles should be preserved by outer cortical bone removal only.
Dr. Barry Eppley
World-Renowned Plastic Surgeon