

Excessively wide cheekbones are a not uncommon facial feature that, although often mainly associated with Asian faces, can occur in all ethnicities. The concept of how wide cheekbones have to be to be considered excessive is an individual one. But anatomically they almost all share a significant or undesired convexity to the anterior portion of the zygomatic arch.
The zygomatic arch makes up a significant amount of the cheekbone and is largely responsible for its external shape. There is the main body the zygoma which is the larger anterior portion. The arch is the thinner bridge of bone that runs between the zygomatic body anteriorly and the temporal bone of the skull posteriorly. The arch is essentially a bridge of bone that has its shape to permit the temporal muscle to pass underneath it as well as is the attachment points for the temporal fascia along its upper border and the masseter muscle at its lower border.
 In anatomical diagrams the zygomatic arch is commonly shown as having an equal convexity from front to back. But the reality is the most convex part of the zygomatic arch is located at the posterior temporal process and it becomes much less convex or almost flat as it approaches the zygomatic body. It has this shape because the bulk of the temporalis muscle that passes underneath the arch is located closer to the ear than to the eye.
In anatomical diagrams the zygomatic arch is commonly shown as having an equal convexity from front to back. But the reality is the most convex part of the zygomatic arch is located at the posterior temporal process and it becomes much less convex or almost flat as it approaches the zygomatic body. It has this shape because the bulk of the temporalis muscle that passes underneath the arch is located closer to the ear than to the eye.
 In patients with wide cheekbones the anterior arch will be wider but never as wide or wider than the posterior arch. Insetting of the zygomatic arch is the fundamental concept behind cheekbone reduction surgery.
In patients with wide cheekbones the anterior arch will be wider but never as wide or wider than the posterior arch. Insetting of the zygomatic arch is the fundamental concept behind cheekbone reduction surgery.

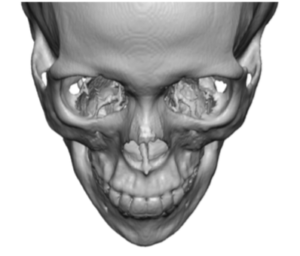
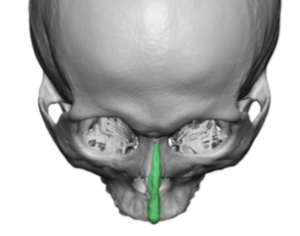
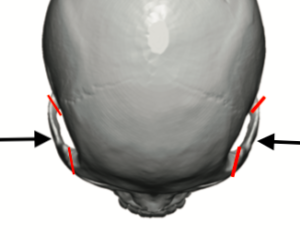
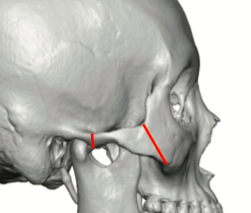
 It typically requires an intraoral osteotomy through the main zygomatic body and an external approach to the posterior arch osteotomy done from an incision in front of the ear. This then allows the entire arch to be moved inward. They are numerous type of anterior osteotomy designs (e.g., oblique, v-shaped) but only one type of posterior arch bone cut. Plate and screw fixation is always used at the intraoral osteotomy and is the important stabilization point. The posterior arch can be stabilized with a plate and screws or an interlocking design can be done which is self-stabilizing. Bur the main role of the posterior arch osteotomy is the allow the anterior part to move inward.
It typically requires an intraoral osteotomy through the main zygomatic body and an external approach to the posterior arch osteotomy done from an incision in front of the ear. This then allows the entire arch to be moved inward. They are numerous type of anterior osteotomy designs (e.g., oblique, v-shaped) but only one type of posterior arch bone cut. Plate and screw fixation is always used at the intraoral osteotomy and is the important stabilization point. The posterior arch can be stabilized with a plate and screws or an interlocking design can be done which is self-stabilizing. Bur the main role of the posterior arch osteotomy is the allow the anterior part to move inward.
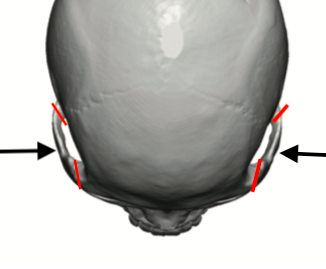
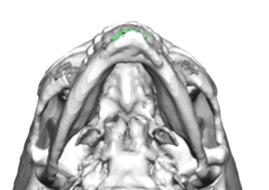
 The inward movement of the zygomatic arch creates the reduction in cheek width which is greater anteriorly than it is posteriorly. (as seen from above with right cheekbone reduction completed and left unoperated.
The inward movement of the zygomatic arch creates the reduction in cheek width which is greater anteriorly than it is posteriorly. (as seen from above with right cheekbone reduction completed and left unoperated.

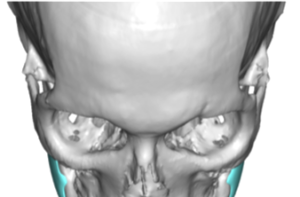
 3D CT scans show the inward movement of the zygomatic arch. A 5mm to 7mm inward movement is typically done. It usually heals by bony consolidation which is more evident anteriorly than the thin arch posteriorly. The inferior location of the plate anteriorly is key, not only for osteotomy stabilization but also to prevent a downward drift of the bone which is one of the key reasons for postoperative soft tissue sagging of the cheek.
3D CT scans show the inward movement of the zygomatic arch. A 5mm to 7mm inward movement is typically done. It usually heals by bony consolidation which is more evident anteriorly than the thin arch posteriorly. The inferior location of the plate anteriorly is key, not only for osteotomy stabilization but also to prevent a downward drift of the bone which is one of the key reasons for postoperative soft tissue sagging of the cheek.
 The inward movement of the zygomatic arch has the capability of compressing the the temporalis muscle since the muscle space underneath the bone is less. While a common problem seen in zygomatic arch fractures (due to the edges of the bone sticking into the muscle from the mod-arch fracture) it is not seen in cheekbone reductions as the entire arch length is intact.
The inward movement of the zygomatic arch has the capability of compressing the the temporalis muscle since the muscle space underneath the bone is less. While a common problem seen in zygomatic arch fractures (due to the edges of the bone sticking into the muscle from the mod-arch fracture) it is not seen in cheekbone reductions as the entire arch length is intact.
Dr. Barry Eppley
Indianapolis, Indiana