


Despite the fact that jaw angle implants have been around almost as long as chin implants, and there are two jaw angles and only one chin, the use of jaw angle implants is but a fraction of that of chin implants. Historically the reason for the limited use of jaw angle implants was demand…few patients requested the procedure. But today the jaw angle region is drawing considerable aesthetic interest, and while some of this patient interest is being fulfilled by injectable fillers, other patients seek a permanent implant solution.
Of all available off-the-shelf facial implants, the jaw angle implant is the most challenging to properly place and malpositions are quite common. Part of this reason is the remote incisional access that its needed way in the back of the mouth. But the main reason is the lack of understanding of the bony anatomy of the jaw angle and their soft tissue attachments.
Many perceive the jaw angle as a flat surfaced piece of the lower jaw that is a smooth extension of the jawline in front of it. And this is certainly how it appears in a panorex x-ray, the most commonly taken jaw x-ray.. But nothing could be further from the anatomic truth.
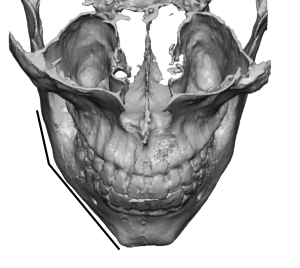
 The first anatomic concept to grasp about the jaw angles, and a major reason for implant malposition, is that it extends much further back than it seems. It is easy to be fooled by the prominence of the external oblique line and to think the back end of the jaw angle is just behind it. But it is not. The angulation of the jaw angles in most patients turns inward at the external oblique line, making the back end or posterior border of the jaw angles difficult to see and straight elevating instruments harder to reach.
The first anatomic concept to grasp about the jaw angles, and a major reason for implant malposition, is that it extends much further back than it seems. It is easy to be fooled by the prominence of the external oblique line and to think the back end of the jaw angle is just behind it. But it is not. The angulation of the jaw angles in most patients turns inward at the external oblique line, making the back end or posterior border of the jaw angles difficult to see and straight elevating instruments harder to reach.
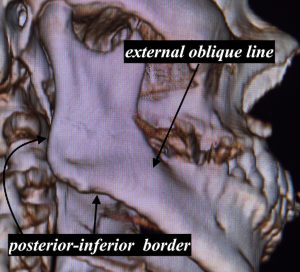
 Between the external oblique line and the posterior border is a concave region which occupies much of the surface area of the jaw angle known as the muscle fossa. This bony recess is where the thickest part of the masseter muscle resides. The muscle attaches at its insertions along the posterior-inferior bony borders after crossing over the concave fossa. It is key in the placement of any jaw angle implant to get the muscle elevated completely off of the fossa to get the implant under it as far back as the bone will permit. It is this failure to get the muscle completely elevated that many jaw angle implants end up too far forward and not sitting in the depth of the fossa.
Between the external oblique line and the posterior border is a concave region which occupies much of the surface area of the jaw angle known as the muscle fossa. This bony recess is where the thickest part of the masseter muscle resides. The muscle attaches at its insertions along the posterior-inferior bony borders after crossing over the concave fossa. It is key in the placement of any jaw angle implant to get the muscle elevated completely off of the fossa to get the implant under it as far back as the bone will permit. It is this failure to get the muscle completely elevated that many jaw angle implants end up too far forward and not sitting in the depth of the fossa.
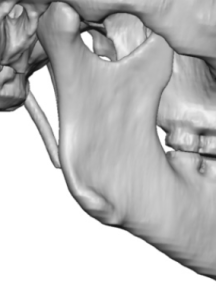
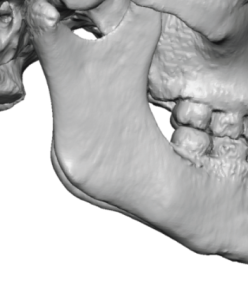 While just getting the muscle adequately elevated is sufficient for most widening jaw angle implants, it is not enough for any type of jaw angle implant that adds vertical length. To get this implant into proper position the muscle attachments along the inferior border must be released…but without disrupting their thin attachments as they wrap around the inferior border and connect with the pterygoid muscle on the inside of the jaw angle. The ability to get the inferior insertion line of the masseter muscle evaluated to permit an implant to go over and beyond it depends on how adherent the ligamentous attachments are to the bone. The 3D CT scan allows the ease or difficulty of doing so to be visualized by the presence or absence of bony spicules or spikes along the inferior border and at the jaw angle point. Strong ligamentous attachments, which are typically seen in most males, have very visible spikes or raised areas where the ligaments are located. Lack of these bony bumps or a more smooth inferior border, which is what is seen in most females, means the ligaments can more easily be elevated as they are not strongly attached.
While just getting the muscle adequately elevated is sufficient for most widening jaw angle implants, it is not enough for any type of jaw angle implant that adds vertical length. To get this implant into proper position the muscle attachments along the inferior border must be released…but without disrupting their thin attachments as they wrap around the inferior border and connect with the pterygoid muscle on the inside of the jaw angle. The ability to get the inferior insertion line of the masseter muscle evaluated to permit an implant to go over and beyond it depends on how adherent the ligamentous attachments are to the bone. The 3D CT scan allows the ease or difficulty of doing so to be visualized by the presence or absence of bony spicules or spikes along the inferior border and at the jaw angle point. Strong ligamentous attachments, which are typically seen in most males, have very visible spikes or raised areas where the ligaments are located. Lack of these bony bumps or a more smooth inferior border, which is what is seen in most females, means the ligaments can more easily be elevated as they are not strongly attached.
The placement of jaw angle implants is not easy but having a good understanding of the bony shape of the angle region and its soft tissue attachments makes for a potential better aesthetic outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon