

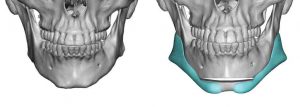
The custom jawline implant is the most effective method of achieving a total jawline augmentation change. Its surface area coverage through its wrap around design alters all aspects of the face-neck transitional area through soft tissue release and expansion from the implant spacer on the bone.
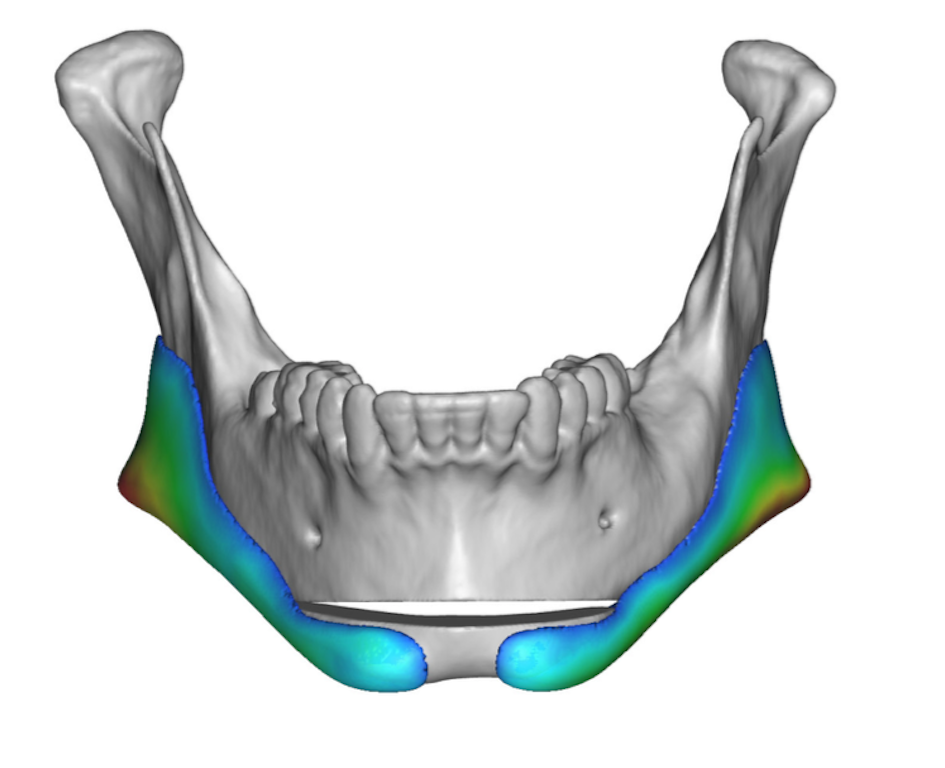
The soft tissue expansion effect of the implant is uniquely felt in the chin area. Since the chin is a solitary projecting point its enveloping soft tissue is tighter than anywhere else along the jawline. As a result one must be cautious as to the implant load placed over the chin to ensure competent wound healing and prevention of excessive long term soft tissue atrophy. The exact volume of implant volume that is safe vs unsafe over the chin varies per each patient. It is the vertical elongation that affects the soft tissue chin pad more than a horizontal augmentation. But when the two are done together one must be extremely aware of these dimensional changes on the overlying soft tissue chin pad.
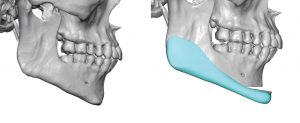
 As a result of this consideration I will occasionally employ a combined autogenous-alloplastic approach to total jawline augmentation when significant vertical elongation of the chin is desired. The primary chin dimensional changes are done by a vertical lengthening bony genioplasty onto which custom extended jawline implants are merged into it to complete the total jawline augmentation effect. This allows the natural chin bone with its attached soft tissues to stretch the chin area out where similar risks associated with implants doing so do not occur.
As a result of this consideration I will occasionally employ a combined autogenous-alloplastic approach to total jawline augmentation when significant vertical elongation of the chin is desired. The primary chin dimensional changes are done by a vertical lengthening bony genioplasty onto which custom extended jawline implants are merged into it to complete the total jawline augmentation effect. This allows the natural chin bone with its attached soft tissues to stretch the chin area out where similar risks associated with implants doing so do not occur.
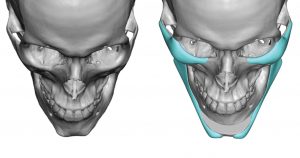
 In this dual jawline augmentation approach implants are an important part of each component but their level of contribution differs. For the bony genioplasty the titanium plates and screws are a supportive part of creating the effect. For the rest of the jawline the custom implant is responsible for the primary effect.
In this dual jawline augmentation approach implants are an important part of each component but their level of contribution differs. For the bony genioplasty the titanium plates and screws are a supportive part of creating the effect. For the rest of the jawline the custom implant is responsible for the primary effect.

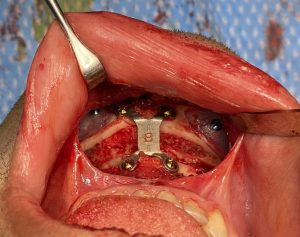
 In executing this procedural combination the vertical lengthening genioplasty is initially performed. It is set and stabilized into the desired amount of vertical lengthening and horizontal advancement desired.
In executing this procedural combination the vertical lengthening genioplasty is initially performed. It is set and stabilized into the desired amount of vertical lengthening and horizontal advancement desired.
 Then the subperiosteal dissection is carried posterior from the end of the bony genioplasy cut and below the mental nerve. Dissection is further completed aided by intraoral posterior vestibular incision. The custom jawline implants are passed from the se incision and brought to their desired position along the side or front end of the bony genioplasty. They attached to the chin by screw fixation. The back end of the implants are secured to jaw angle bone by percutaneous screw fixation.
Then the subperiosteal dissection is carried posterior from the end of the bony genioplasy cut and below the mental nerve. Dissection is further completed aided by intraoral posterior vestibular incision. The custom jawline implants are passed from the se incision and brought to their desired position along the side or front end of the bony genioplasty. They attached to the chin by screw fixation. The back end of the implants are secured to jaw angle bone by percutaneous screw fixation.
 Lastly tissue bank bone chips that have been soaked in an antibiotic solution are placed into the gap and step off of the genioplasty to obliterate the bony gap and cover the fixation plate. All three intraoral incisions are then closed in multiple layers.
Lastly tissue bank bone chips that have been soaked in an antibiotic solution are placed into the gap and step off of the genioplasty to obliterate the bony gap and cover the fixation plate. All three intraoral incisions are then closed in multiple layers.
Taking advantage of the best properties of various lower jaw reshaping techniques, the combination of a chin osteotomy and custom implants for the rest of the jaw can be effectively used. The computer design process allows the implants to merge into the planned bony genioplasty in a predictable manner for a smooth jawline feel. This also conveniently obscures the step off from the back end of the bony genioplasty as well.
Dr. Barry Eppley
Indianapolis, Indianapolis