

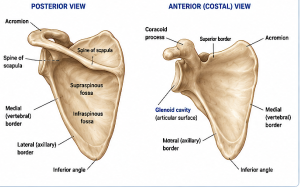
The scapula (shoulder blade) is a flat triangular bone that connects the arm to the trunk through muscular and ligamentous attachments. It serves as the mobile platform for shoulder motion.
Key anatomical regions include:
- Spine of scapula
Prominent ridge on the posterior surface dividing:- supraspinous fossa
- infraspinous fossa
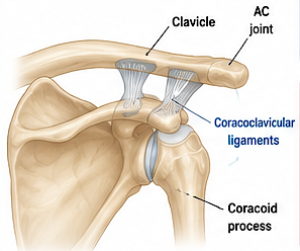
- Acromion
- Extension of the scapular spine
- Forms the AC joint with the clavicle
- Coracoid process
- Hook-like anterior projection
- Attachment for:
- pectoralis minor
- short head of biceps
- coracobrachialis
- coracoclavicular ligaments
- Glenoid
- Shallow socket articulating with the humeral head
- Forms the glenohumeral joint
- Medial (vertebral) border
- Attachment for rhomboids and serratus anterior interaction
- Inferior angle
- Important landmark for scapular rotation
- Lateral border
- Attachment for teres major and teres minor
Important muscle relationships:
- Trapezius – elevation/upward rotation
- Serratus anterior – protraction/upward rotation
- Rhomboids – retraction
- Levator scapulae – elevation
- Rotator cuff muscles originate from scapular fossae
Normal scapular motion includes:
- elevation/depression
- protraction/retraction
- upward/downward rotation
- anterior/posterior tilt
The clavicle strongly influences scapular position because the scapula is suspended from it through the AC joint and coracoclavicular ligaments.
How then is the scapula affected in clavicle bone shortening surgery?
In clavicle shortening surgery for shoulder narrowing, the scapula is indirectly affected because the clavicle acts as a strut that holds the shoulder girdle away from the chest wall. When the clavicle is shortened, the scapula tends to shift position.


The key biomechanical effects on the scapula are:
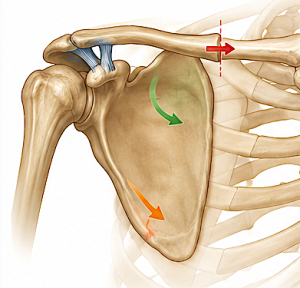
- Scapular protraction
-
- The scapula slightly moves forward and around the rib cage.
- Scapular downward rotation
-
- The inferior angle may move medially/downward.
- Medialization of the shoulder girdle
-
- The entire shoulder complex sits closer to the sternum.
- Shoulder width decreases
- Potential scapular winging
-
- Will only develop if shortening is substantial which is beyond the amount of clavicle bone removed
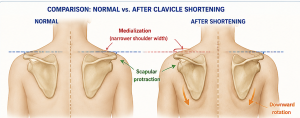
Biomechanical studies show that shortening beyond about 20–25 mm is well tolerated in terms of scapular orientation and shoulder function.
The scapula and clavicle are tightly linked through the:
- acromioclavicular (AC) joint
- coracoclavicular ligaments
- scapuloclavicular muscle balance
So changing clavicle length inevitably repositions the scapula but those changes are slight within the amount of clavicle shortening that is technically possible
Dr Barry Eppley
Plastic Surgeon