

The buccal lipectomy is the most well known soft tissue cheek reduction procedure. While it can provide effective reduction of fuller cheeks, the extent of its effect is frequently misunderstood or overstated. (leading to unfulfilled patient expectations)

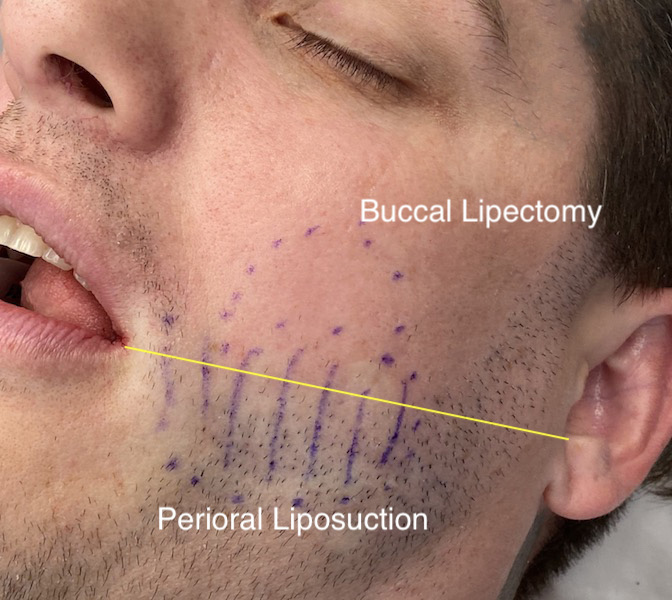
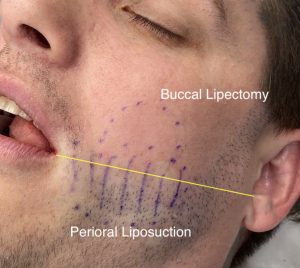 The effect of the buccal lipectomy is best understood by where it is positioned in the midface. Sandwiched between the masseter and pterygoid muscles and bordered posteriorly by the temporalis muscle and the buccinator muscle inferiorly, its effect can not by anatomic definition extend lower than the level of the maxillary teeth or occlusal plane. This is best appreciated externally by drawing a line from the attachment of the earlobe to the corner of the mouth. Any desired effect below this line will not occur from a buccal lipectomy in most patients.
The effect of the buccal lipectomy is best understood by where it is positioned in the midface. Sandwiched between the masseter and pterygoid muscles and bordered posteriorly by the temporalis muscle and the buccinator muscle inferiorly, its effect can not by anatomic definition extend lower than the level of the maxillary teeth or occlusal plane. This is best appreciated externally by drawing a line from the attachment of the earlobe to the corner of the mouth. Any desired effect below this line will not occur from a buccal lipectomy in most patients.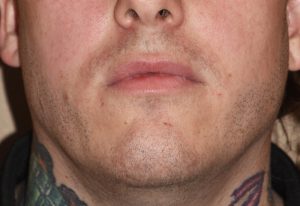

Because of the limited extent of the buccal lipectomy in reducing overall cheek fullness, the role of perioral fat reduction becomes aesthetically important. This is the subcutaneous fat layer that exists between the buccinator muscle and the skin. (and technically between the buccinator muscle and the intraoral mucosa as well) Reduction of this fat layer, while never magnaminous in effect due to low fat volumes, does provide a visible thinning effect below the level of what the buccal fat pad removal does.
Small cannula perioral liposuction is most typically in my experience a complement to the buccal lipectomy procedure. It creates a more complete soft tissue cheek reduction effect. In some cases of isolated perioral mound treatment it is the definitive treatment for it.
While small in fat volume treatment of the perioral region is often over looked. It is often attempted to be reduced by injectable therapies but not often unsuccessful due to the fibrofatty nature of the tissues being a low metabolic fat site.
Dr. Barry Eppley
Indianapolis, Indianapolis