

The extremities are capable of undergoing aesthetic muscle augmentation using implants of which the most commonly done historically is that of calf implants. Today other extremity augmentations are also done in the upper arm for biceps and tricep implants.
What all of these extremity implantation sites share is that of a muscle which glides inside of its enveloping fascial sheath. This is necessary for the elongation and contraction of the muscle which contributes to extremity extension and flexion. This is relevant for implant placement because it means the muscle is not adhered to the fascia. This makes it possible to develop a subfascial pocket on top of the muscle in a relatively atraumatic fashion.
Besides the gastrocnemius, bicep and tricep muscles there are other extremity muscles that share this trait that can also be augmented with an implant. One such lower extremity area is that of the upper leg or thigh. Patients may seek augmentation of the thigh for either aesthetic reasons, because they are too thin, or for reconstructive reasons due to muscle atrophy. For either reason the implantation site is the quadricep muscle, specifically the rectus femoris.
The rectus femoris is the largest quadricep muscle of the anterior thigh. Its origin is on the hip at the anterior iliac spine and it extends down to insert onto the patella. Due to long tendinous attachments from the hip the muscle only covers the lower two-thirds of the anterior thigh. It has a fusiform shape and occupies the largest surface area of any of the seven anterior thigh muscles.


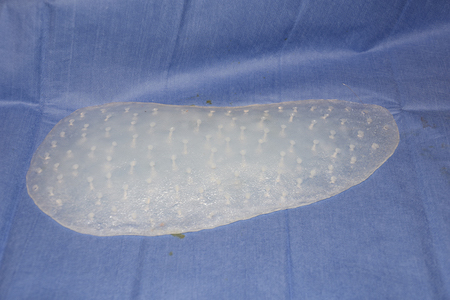
 Access to the muscle is typically done through a small high anterolateral skin incision. In reconstructive cases it may be done through an existing incision/scar if one exists on the thigh. Subfascial dissection is how the pocket is made. There are no standard thigh implants or any standard body implant that will suffice for this application. Most thigh implants are in the 24 to 26cm lengths and 10 to 12 cms width…but in a fusiform shape which is consistent with the natural shape of the muscle. This will be a fairly tight pocket so maximum implant height is no more than 1.0 to 1.5cms.
Access to the muscle is typically done through a small high anterolateral skin incision. In reconstructive cases it may be done through an existing incision/scar if one exists on the thigh. Subfascial dissection is how the pocket is made. There are no standard thigh implants or any standard body implant that will suffice for this application. Most thigh implants are in the 24 to 26cm lengths and 10 to 12 cms width…but in a fusiform shape which is consistent with the natural shape of the muscle. This will be a fairly tight pocket so maximum implant height is no more than 1.0 to 1.5cms.
Closure of the fascia can be done if it is not unduly tight. But otherwise there is no reason to do so as the implant can not slide out of the pocket. Very tight fascial closure leads to prolonged postoperative pain and thigh stiffness. It is important to remember that the fascia developed without having an implant in place. Thus ‘decompression’ may be needed by leaving the fascia open.
I usually do not use a drain and the thighs have only ace wraps or lightly wrapped coban elastic wraps placed for dressings. Patients will continue to wear these wraps as long as their use is associated with greater comfort than not wearing them. Patients should begin walking, bending and doing knee extensions as soon as they feel comfortable in beginning to do so.
Dr. Barry Eppley
Indianapolis, Indiana