

Shoulder feminization surgery is done by surgical shortening of the clavicles. (clavicular reduction osteotomies) Since clavicles provide horizontal spacing between the sternum and the shoulder, it is easy to see how shortening their length provides reduction in bideltoid shoulder width measurements and appearance. Even though the clavicle is not a pure horizontal rod of bone, shortening its lazy S-shape still primarily produces a horizontal width reduction effect.

 The key question of the surgery, and one patients frequently ask, is how much clavicle bone can be taken to get a good aesthetic result. Most of the time 2.0 to 2.5cms of clavicle is taken per side, resulting in close to 5 cms or two inches in total or bilateral shoulder width reduction. This amounts to about 15% to 18% length reduction considering the average clavicle length in a male is 16 cms and 14cms in a female.
The key question of the surgery, and one patients frequently ask, is how much clavicle bone can be taken to get a good aesthetic result. Most of the time 2.0 to 2.5cms of clavicle is taken per side, resulting in close to 5 cms or two inches in total or bilateral shoulder width reduction. This amounts to about 15% to 18% length reduction considering the average clavicle length in a male is 16 cms and 14cms in a female.
Patients not infrequently ask whether more can be taken and this is a question that can be answered two ways….1) At what point in clavicle reduction will shoulder function be affected, and 2) at what shoulder width does it appear feminine? From the orthopedic literature looking at clavicle fractures, the general range of around 30% or greater loss of clavicle length can begin to affect shoulder function and stability. So based on this criteria the number of up to 3.5cms would be considered safe. (25% length reduction)
 From an aesthetic standpoint anthropometric studies have evaluated shoulder width gender differences. Bideltoid width measurements are the most useful as they are a practical measure of viewed shoulder width as it includes the deltoid muscle thickness. These studies have shown that bideltoid width measurements of 49 cms or greater are generally masculine in appearance. It takes a 4cm width reduction (2cms per side) to reach 45cms which is more feminine. Thus the concept of taking 2.5cm per side, or a 5cm bideltoid width reduction, should be sufficient to achieve the primary goal of the surgery. (shoulder feminization effect) This would indicate that while more clavicle length could be taken there is no compelling reason to do so.
From an aesthetic standpoint anthropometric studies have evaluated shoulder width gender differences. Bideltoid width measurements are the most useful as they are a practical measure of viewed shoulder width as it includes the deltoid muscle thickness. These studies have shown that bideltoid width measurements of 49 cms or greater are generally masculine in appearance. It takes a 4cm width reduction (2cms per side) to reach 45cms which is more feminine. Thus the concept of taking 2.5cm per side, or a 5cm bideltoid width reduction, should be sufficient to achieve the primary goal of the surgery. (shoulder feminization effect) This would indicate that while more clavicle length could be taken there is no compelling reason to do so.
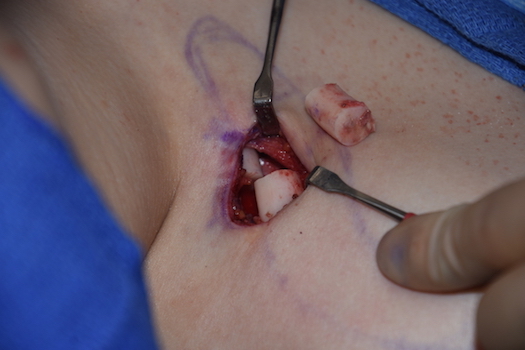
Classic length reductions of 2.5cms per side have proven to result in uncomplicated healing with no evidence of bony non-unions or shoulder dysfunction in my experience. Based on body size it may be that 3cms per side may be more considered in taller/larger patients.
Dr. Barry Eppley
Indianapolis, Indiana