

Facelift surgery is well known to lift, remove and tighten skin that is recruited from the jowls and neck. In its most simplest form, a facelift chases sagging and loose skin from the neck and jawline back to where its removal offers the best incision placement and resultant scar creation…in and around the ears. In its infancy, facelift surgery was all about just removing skin and the wrinkles that it contained, hence the original name of rhytidectomy. (the removal of rhytids or wrinkles)
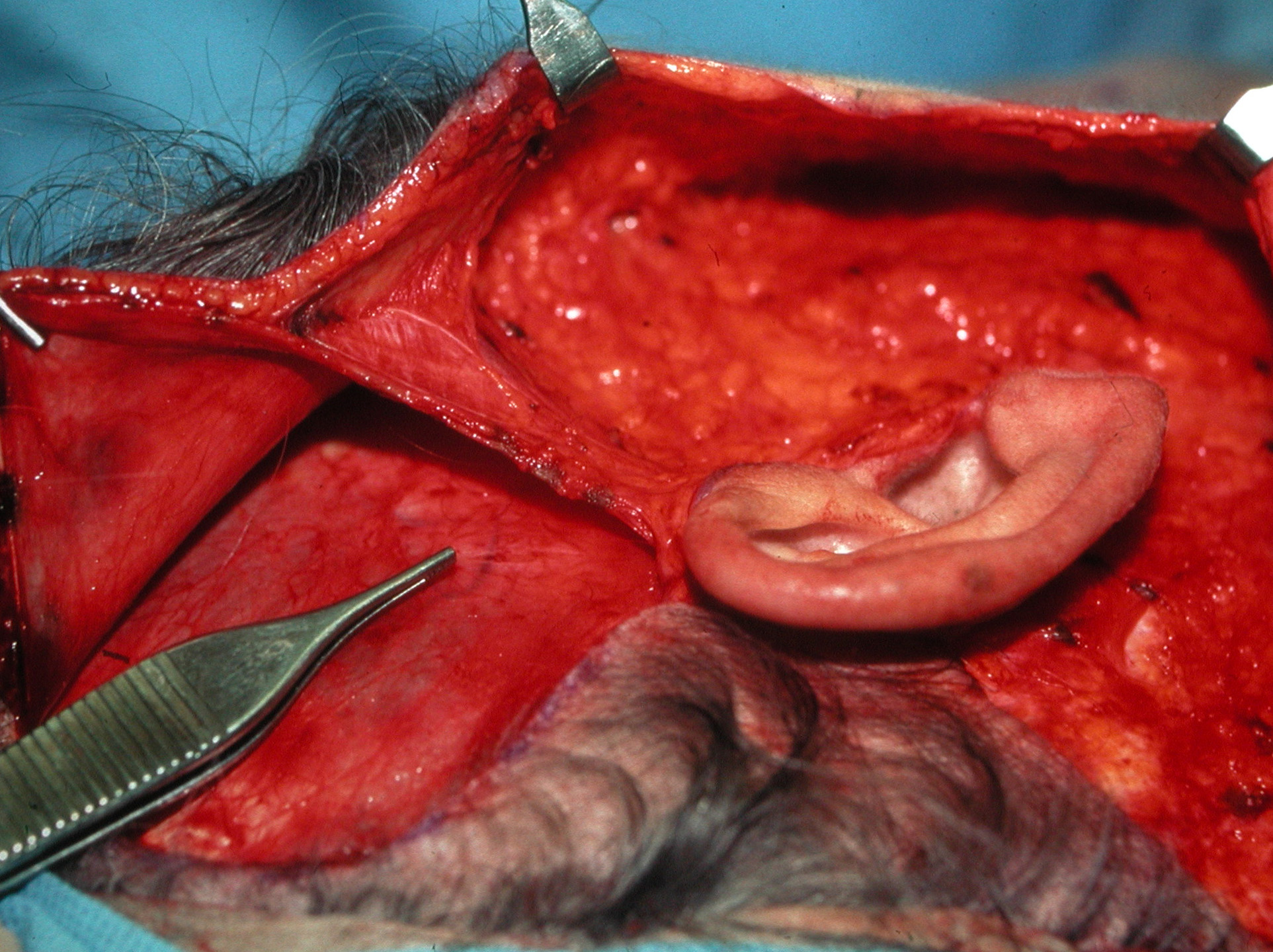
But for decades the lifting of an aging face has gone deeper to involve more than just skin. A layer under the skin, known by the acronym SMAS (submusculoaponeurotic system), has been lifted as well. The ability to provide deep lifting to the SMAS of the face increases the longevity of a facelift’s effects and helps reduce skin surface irregularities such as abnormal looking pull lines and other facial distortions.
The concept of SMAS modifications in facelifts has undergone a tremendous amount of scrutiny from anatomic dissections published in journals to endless roundtable discussions at innumerable plastic surgery meetings. Some plastic surgeons endorse its most extensive use and these procedures are generally called ‘deep-plane facelifts’. Other plastic surgeons have an opposite approach and use minimal to no manipulation of the SMAS in their facelifts based on the premise of a quicker and less complicated surgery. It is this group of facelifts that have the most diverse number of monikers such as Lifestyle Lifts and Quicklifts to name a few.
 The trend in SMAS facelifts today has trended back now to the concept of less is more. The raising of an extensive SMAS flap, once the gold standard in facelift surgery, is not so today. SMAS techniques are more about limited deep undermining or more simple lifting and tightening it by sutures alone. (imbrication) The more rapid and safer execution of this part of a facelift is a big reason for this trend. There is very little chance of nerve injury and the bulk or volume of the face is preserved. This is particularly advantageous in the thin patient with little SMAS thickness anyway.
The trend in SMAS facelifts today has trended back now to the concept of less is more. The raising of an extensive SMAS flap, once the gold standard in facelift surgery, is not so today. SMAS techniques are more about limited deep undermining or more simple lifting and tightening it by sutures alone. (imbrication) The more rapid and safer execution of this part of a facelift is a big reason for this trend. There is very little chance of nerve injury and the bulk or volume of the face is preserved. This is particularly advantageous in the thin patient with little SMAS thickness anyway.
In the past I would do a SMAS elevation underneath the facial skin is thick or heavier patients and do only a SMAS imbrication in thinner patients. But in looking at the results months later it was impossible to tell the difference between the two SMAS techniques. So today I just perform a good SMAS imbrication on all facelift patients. Their recovery is quicker and the results appear to be just as good.
The time saved from doing deep SMAS lifting is now spent on other adjunctive facial procedures that add more benefits to the overall facelift procedure. This is usually fat injections around the mouth and nasolabial folds and skin resurfacing with the fractional laser or chemical peels.
Dr. Barry Eppley
Indianapolis, Indiana