

As one ages, the upper lip may get longer or one may have a long upper lip naturally. When one is dissatisfied with lack of upper lip fullness (vermilion show) and has a long upper lip, only skin excisional procedures can address both problems.
Skin can be removed through two classical upper lip operations. When skin is taken low, the short vermilion is advanced upward encompassing its name, vermilion or lip advancement. When skin is taken high (under the nose) the upper lip skin is pulled upwards appropriately named a subnasal or a bullhorn (because of the shape of the skin cutout) liplift. Each approach has its advantages and disadvantages. In either case, one has to be sure that the trade-off of a scar is better lip ‘problem’ than that of too much upper lip skin and a thin vermilion.
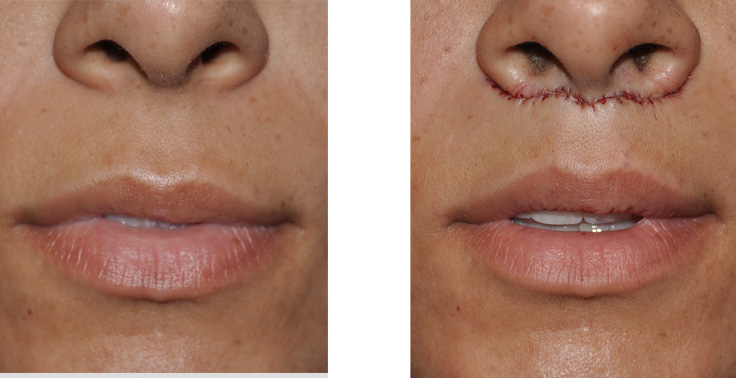 In the lip lift procedure, a wavy amount of skin (thicker in the middle) is taken directly beneath the nose with advancement of the lower edge of the incision to the area directly beneath the nose. The final closure is tucked in along the base of the nose from one side of the nostril to the other. This procedure shortens the distance between the top lip and the tip of the nose allowing for more upper tooth show when the lips are slightly parted. It also everts more of the upper lip vermilion, therefore creating more of a central pout of the upper lip. It is always slightly overcorrected as there will be some relaxation (mild re-lengthening) of the upper lip afterwards.
In the lip lift procedure, a wavy amount of skin (thicker in the middle) is taken directly beneath the nose with advancement of the lower edge of the incision to the area directly beneath the nose. The final closure is tucked in along the base of the nose from one side of the nostril to the other. This procedure shortens the distance between the top lip and the tip of the nose allowing for more upper tooth show when the lips are slightly parted. It also everts more of the upper lip vermilion, therefore creating more of a central pout of the upper lip. It is always slightly overcorrected as there will be some relaxation (mild re-lengthening) of the upper lip afterwards.
While this is a fairly simple procedure, I have seen and read of some problems associated with it. One complication appears to be from manipulating the underlying orbicularis oris muscle besides the skin while doing the upper lip lift. In theory, sewing the orbicularis oris muscle to the periosteum underneath the nose may make for a more stable long-term result. However,such a maneuver creates an unnatural stiffness and deformity of the upper lip when can be evident during smiling. It may also cause the nose to move unnaturally. This is not a fundamentally good trade-off for its purported benefits. It is far better to run the inconsequential risk of doing a secondary tuck-up the procedure if there has been some relapse. Correction of this problem can be done with re-opening the incision and releasing the abnormal attachments, with the possible insertion of a dermal or dermal-fat graft to prevent recurrence.
In an effort to hide the scars more obscurely, some lip lift techniques advocate moving the scars within the nostril opening. This sounds theoretically beneficial but it can easily cause distortion of the sill of the nostril resulting in enlargement of the nostril openings and distorted sill anatomy. The nostril sill is not generally paid too much attention (except in cleft lip repairs) but it is easily altered and then becomes a lot more noticeable. It is best not to mess with this part of the nostril anatomy. Secondary correction is difficult.
The last complication that has been reported is a distortion of the nostril but being pulled downward by scar contracture afterwards. This is the result of removing too much skin (a few extra millimeters is all that it takes) underneath the nostril. This is why the cutout is wavy with the greatest amount taken between the philtrums. Since skin can not be easily replaced, secondary correction can be attempted by a modification of the inner alar wedge technique.
Upper lip lifts can be a very satisfying procedure but it is important to not try and take too much skin or get ‘too fancy’ with it. In my Indianapolis plastic surgery practice, I take a central 4 -5 mms of skin removal whose pattern tapers out to the lateral alar rim. This approach produces consistent results with negligible risks of any of the aforementioned complications.
Dr. Barry Eppley
Indianapolis, Indiana