

The labiomental fold is a transverse indentation that makes a separation between the upper lip and chin. Its depth differs amongst people in which it can be quite shallow or very deep partially influenced by the development of the lower jaw and the upper and lower incisor tooth relationship. Three muscles help create the fold including the orbicular oris just above it, the mentalis muscle directly underneath it and the inferior depressor muscle crossing its sides. The dominant muscle that contributes most to the depth of the labiomental fold is the mentalis with its deep origin to the bone directly beneath it.
By definition an intraoral approach for chin implant placement or for a sliding genioplasty requires passing through the mentalis muscle beneath the fold. During closure it is necessary to suture back the mentalis muscle that was separated just below its bony origin. This always has the potential to cause muscle stiffness as well as vestibular mucosal and lower lip tightness. In more severe scarring cases it can also lead to lower lip retraction and incompetence. All of these symptoms invariably involve some degree of labiomental tightness and even deepening in more severe cases.
Labiomental fold tightness is not uncommon after intraoral chin surgery. It is usually a self-resolving problem with time and healing. More prolonged cases can be treated by steroid, 5-FU, and PRP injections. Failure to significantly improve with these injections methods may need a more aggressive approach with synthetic injectable fillers or fat injections for volumetric expansion. These approaches will provide good improvement for most labiodental fold tightness patients.
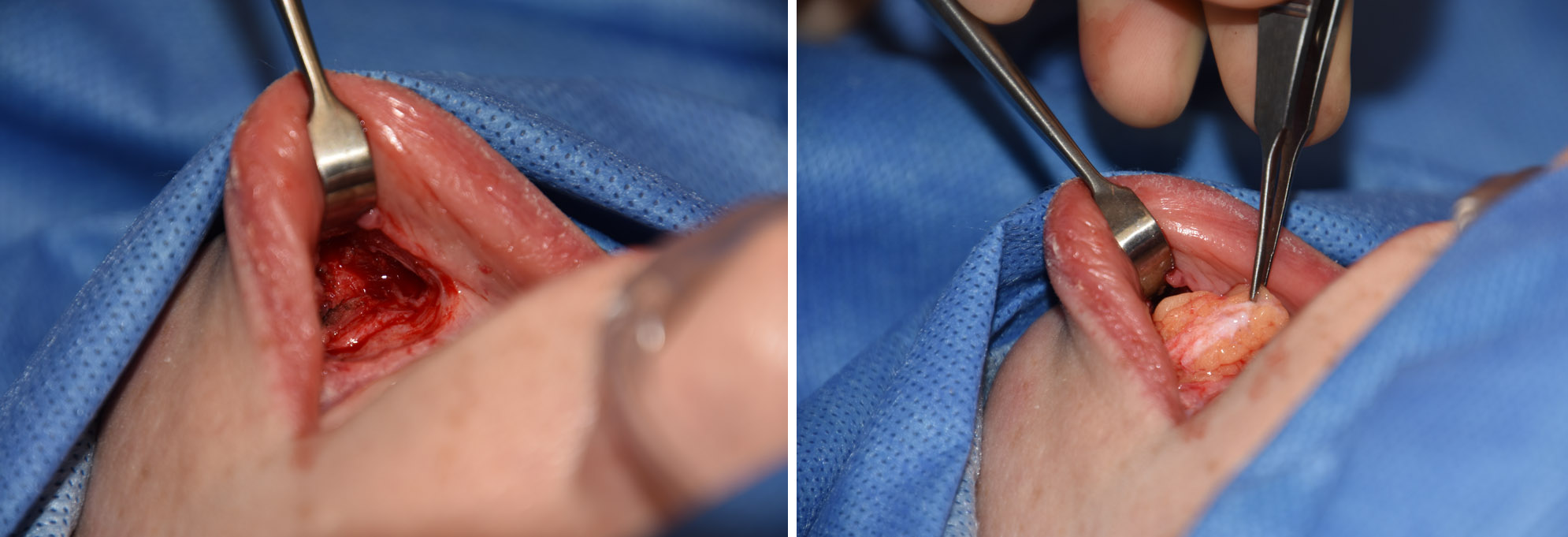
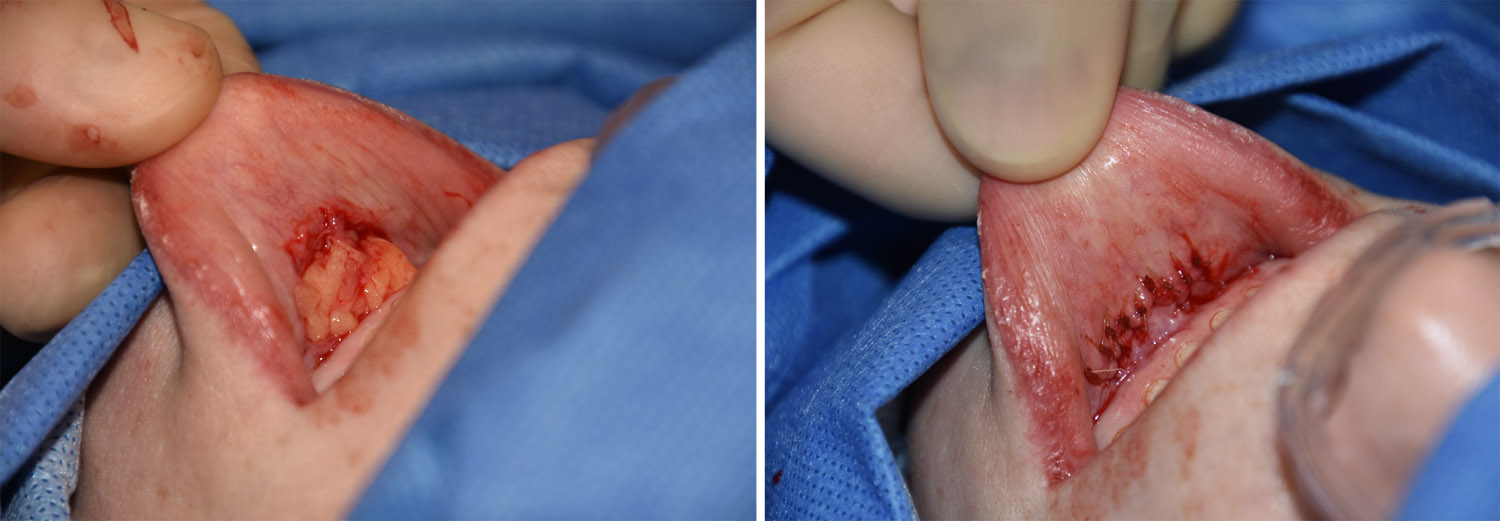 But in severe cases of labiomental fold tightness or contracture, an interpoitional soft tissue graft is the approach. Using either a small dermal-fat graft or an enbloc fat graft, the labiomental fold is released beneath the dermis and above the level of the mentalis muscle across its width. The fat graft is placed (dermal side up if a dermal-fat graft) and the mucosal closed over it.
But in severe cases of labiomental fold tightness or contracture, an interpoitional soft tissue graft is the approach. Using either a small dermal-fat graft or an enbloc fat graft, the labiomental fold is released beneath the dermis and above the level of the mentalis muscle across its width. The fat graft is placed (dermal side up if a dermal-fat graft) and the mucosal closed over it.
Like all adverse scarring and contracture problems n the body, it is ultimately a problem of inadequate tissue quality and quantity. Releasing the tight tissues and placing an interopositional graft is a helpful strategy that directly addresses the primary problem.
In releasing and grafting underneath the labiodental fold, improved lower lip mobility and even lower lip elevation can be seen. No dysfunction of the lower lip has occurred nor would be expected given the graft’s plane of placement. How much of the fat graft survives can not be precisely predicted by such small fat grafts have a long history of good take and retention.
Dr. Barry Eppley
Indianapolis, Indiana