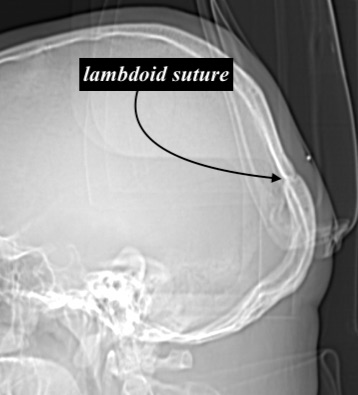


The back of the head is typically called the occiput or occipital bone. But anatomically this is inaccurate as only the lower central part of the back of the head is the occipital bone. Much of the back of the head is the parietal bone which lies above the inverted v-shaped lambdoid sutures.
 Appreciating the location of the occipital bone can be seen when a patient presents that has true occipital bone hypertrophy. This causes a very distinct protrusion on the lower back of the head which emanates onward from the lambdoidal suture line. The location of the suture line can actually be seen as the transition between the lower occipital bone and the more superior paired parietal bones. Why an isolated occipital bone protrusion occurs is not known but it does not appear to be related to malformations of the lambdoid sutures.
Appreciating the location of the occipital bone can be seen when a patient presents that has true occipital bone hypertrophy. This causes a very distinct protrusion on the lower back of the head which emanates onward from the lambdoidal suture line. The location of the suture line can actually be seen as the transition between the lower occipital bone and the more superior paired parietal bones. Why an isolated occipital bone protrusion occurs is not known but it does not appear to be related to malformations of the lambdoid sutures.
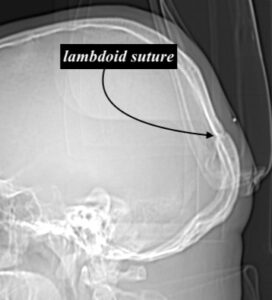 The key surgical question is not whether the occipital bone protrusion can be reduced but whether it can be done so with a complete resolution to a normal looking head shape. A lateral skull film will allow a preoperative assessment to be done looking at the thickness of the bone, knowing that preservation of the inner cortical bone layer needs to be done.
The key surgical question is not whether the occipital bone protrusion can be reduced but whether it can be done so with a complete resolution to a normal looking head shape. A lateral skull film will allow a preoperative assessment to be done looking at the thickness of the bone, knowing that preservation of the inner cortical bone layer needs to be done.
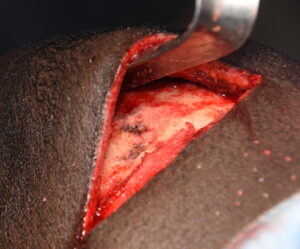 In reducing the occipital bone expect a large amount of bone dust to be created. This is the equivalent of harvesting a large outer cortical table skull bone graft…but in very miniaturized particles. Scraping out the bone dust as the burring reduction is being done requires frequently starting and stopping to do so. And it is important to thoroughly rinse out all loose bone dust at the end.
In reducing the occipital bone expect a large amount of bone dust to be created. This is the equivalent of harvesting a large outer cortical table skull bone graft…but in very miniaturized particles. Scraping out the bone dust as the burring reduction is being done requires frequently starting and stopping to do so. And it is important to thoroughly rinse out all loose bone dust at the end.

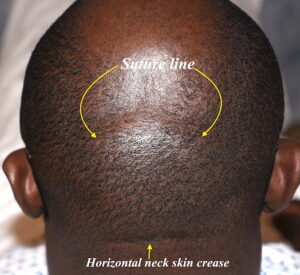
 When closing the scalp incision over a large occipital bone reduction it is important to check for any scalp redundancy. It may be necessary to remove some scalp from the superior side of the incision to avoid the potential for a soft tissue scalp roll to remain when it heals. When both the protruding bone and any scalp excess is removed a good head reshaping result can be obtained.
When closing the scalp incision over a large occipital bone reduction it is important to check for any scalp redundancy. It may be necessary to remove some scalp from the superior side of the incision to avoid the potential for a soft tissue scalp roll to remain when it heals. When both the protruding bone and any scalp excess is removed a good head reshaping result can be obtained.
The occipital bone, by virtue of its location and numerous muscular attachments, is the thickest of all the skull bones. More bone reduction is possible there than, for example, on the front of the skull. (forehead) So substantial occipital skull bone protrusion is always possible.
Dr. Barry Eppley
Indianapolis, Indiana