

Background: The male chest is largely defined by the size and shape of the pectoralis muscle as well as the nipple-areolar complex. While chest asymmetry to some degree is common in many men, significant asymmetry is most commonluy caused by abnormal development. A variety of congenital male chest conditions exist including pectus excavatum and pectus carinatum as the most common occurring 1 to 400 to 1500 births.
Poland’s syndrome was described more than a hundred years ago is fairly rare occurring in more than 1 to 20,000 births. It really describes a spectrum of anterior chest wall deformities that can include the pectoralis major, pectoralis minor, serratus muscles as well as that of the ribs and even potentially extending to involve the arm and hand., ribs, and soft tissue. Deformities of the arm and hand may also be observed. It is far more common in men with a high ride sided occurrence. Poland’s syndrome presents in a wide ranging degree of expression from ver mild chest asymmetry with no arm involvement to the extreme of a flail chest and a short dysfunctional arm.
Reconstruction of many male Poland’s patients involves restoring/recreating the deficient pectoralis major muscle. This has been done historically by implants, muscle flaps and, more recently, fat injections. Each method has their own advantages and disadvantages as well as their own advocates. For smaller pectoral muscle deficiencies the choice of implants vs fat grafting are the logical (benefit vs risk) choices.
Case Study: This 30 year-old male was born with a mild manifestation of Poland’s syndrome that involved the left side of his chest. It was most evident by the loss of a well defined lower pectoralis major muscle border and smaller chest contour. A custom designed implant was made using a silicone elastomer molding technique and send for fabrication into a solid but flexible implant.
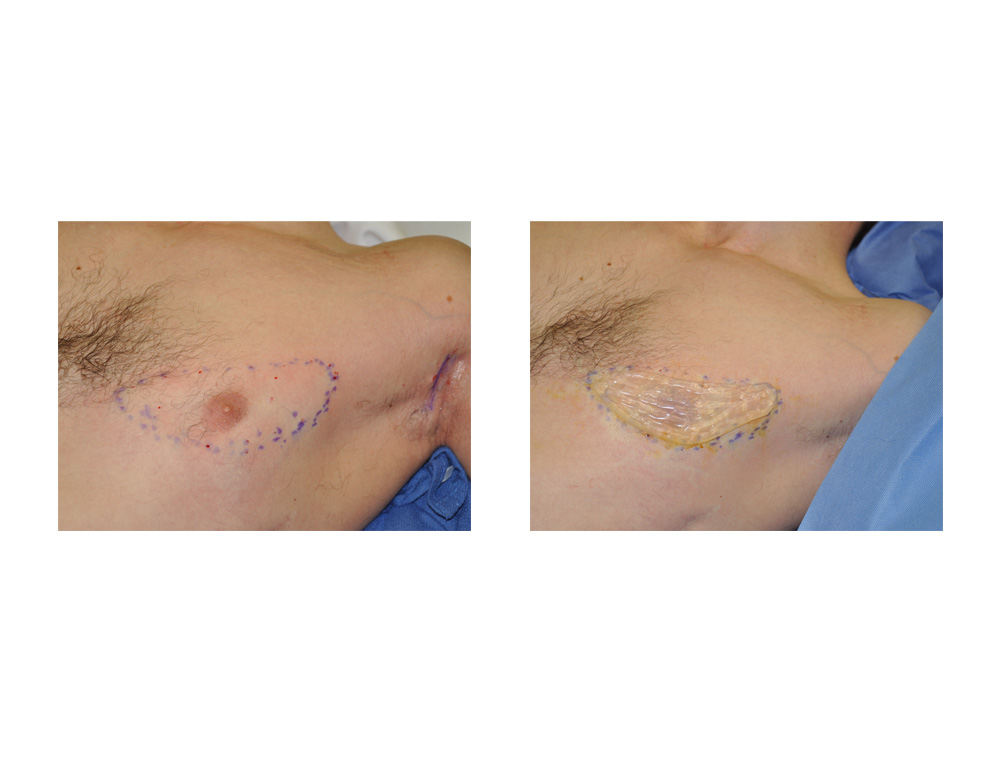 Under general anesthesia, the custom designed pectoral implant was placed through a transaxillary incision. After multiple trial fits it was determined that it was slightly too big. It was reduced down in size using scissors. Using a copy of the location of the lower border of the pectoralis major muscle the implant was inserted into a carefully made pocket using a long dingman dissecting instrument. The limits of the pocket defined the final implant’s location so that it could not migrate either inferiorly or superiorly.
Under general anesthesia, the custom designed pectoral implant was placed through a transaxillary incision. After multiple trial fits it was determined that it was slightly too big. It was reduced down in size using scissors. Using a copy of the location of the lower border of the pectoralis major muscle the implant was inserted into a carefully made pocket using a long dingman dissecting instrument. The limits of the pocket defined the final implant’s location so that it could not migrate either inferiorly or superiorly.
 When seen six months after surgery he had much improved chest asymmetry and no detection that there was any implant in place. It looked perfectly natural . The lower border of the pectoralis major muscle has been restored.
When seen six months after surgery he had much improved chest asymmetry and no detection that there was any implant in place. It looked perfectly natural . The lower border of the pectoralis major muscle has been restored.
Custom designed pectoral implants can provide a good method of Poland’s chest reconstruction but they must be designed properly and placed into a carefully made pocket. There are multiple ways to create a custom designed pectoral implant but the simplest, and probably most effective, is to make a silicone elastomer mold on the actual patient. The muscle deficiency must be carefully determined through arm motion with an understanding that it is very easy to oversize it.
Highlights:
1) Male chest asymmetry is not that common and one of the origins of it is Poland’s syndrome.
2) Reconstruction of the male Poland’s chest is to create pectoralis muscle volume and a defined lower muscular border.
3) A custom designed pectoral implant is a useful reconstructive method in the male Poland’s chest and often needs to be smaller than one would initially think.
Dr. Barry Eppley
Indianapolis, Indiana