

Background: Cleft lip and palate is one of the most common congenital facial deformities. While much focus is on the lip, alveolus and palate, the nose is equally affected as well. While the nose may not be ‘clefted’, deformity underneath it causes a variety of septal, turbinate and nasal cartilage and bone structural alterations.
Management of the nasal portion of a unilateral cleft lip and palate deformity is done at various stages of development. During the primary cleft lip repair, the base of the nose is realigned and in some techniques the nasal tip cartilages are manipulated as well. Prior to or during the early years of school a second effort on the cleft nose is often done. This is done through an open rhinoplasty with emphasis on the reshaping of the deranged nasal tip and cleft sided nostril.
The third opportunity to treat the cleft nose is in the teenage years. Patients are most motivated to have their nose reshaped during these important psychosocial development years. It can be debated as to whether this is done during the early or late teenage years and some plastic surgeons will await until near complete facial growth at age 17 or 18 years old.
Case Study: This 15 year-old hispanic teenager was borne with a unilateral (right) cleft lip and palate. She had prior effort on her nose both at the first few months after birth at the time of cleft lip repair as well as at age 7. By the time she was a teenager, her nose had developed the appearance of a nasal hump as well as the tip showing ipsilateral alar rim collapse and nostril widening.
 Under general anesthesia, a small rib graft (#9) was harvested through a small (3 cm) subcostal cartilage graft. Then an open rhinoplasty was used to access the nasal cartilages and the septal deviation corrected.The nasal tip was lifted using a combination of a strong columellar strut and suture plication to the septum. An alar batten cartilage graft was attached to the dome and columellar strut to give the nostril better support. The remaining rib graft was used to create paranasal augmentation under the base of the cleft-sided nostril.
Under general anesthesia, a small rib graft (#9) was harvested through a small (3 cm) subcostal cartilage graft. Then an open rhinoplasty was used to access the nasal cartilages and the septal deviation corrected.The nasal tip was lifted using a combination of a strong columellar strut and suture plication to the septum. An alar batten cartilage graft was attached to the dome and columellar strut to give the nostril better support. The remaining rib graft was used to create paranasal augmentation under the base of the cleft-sided nostril.


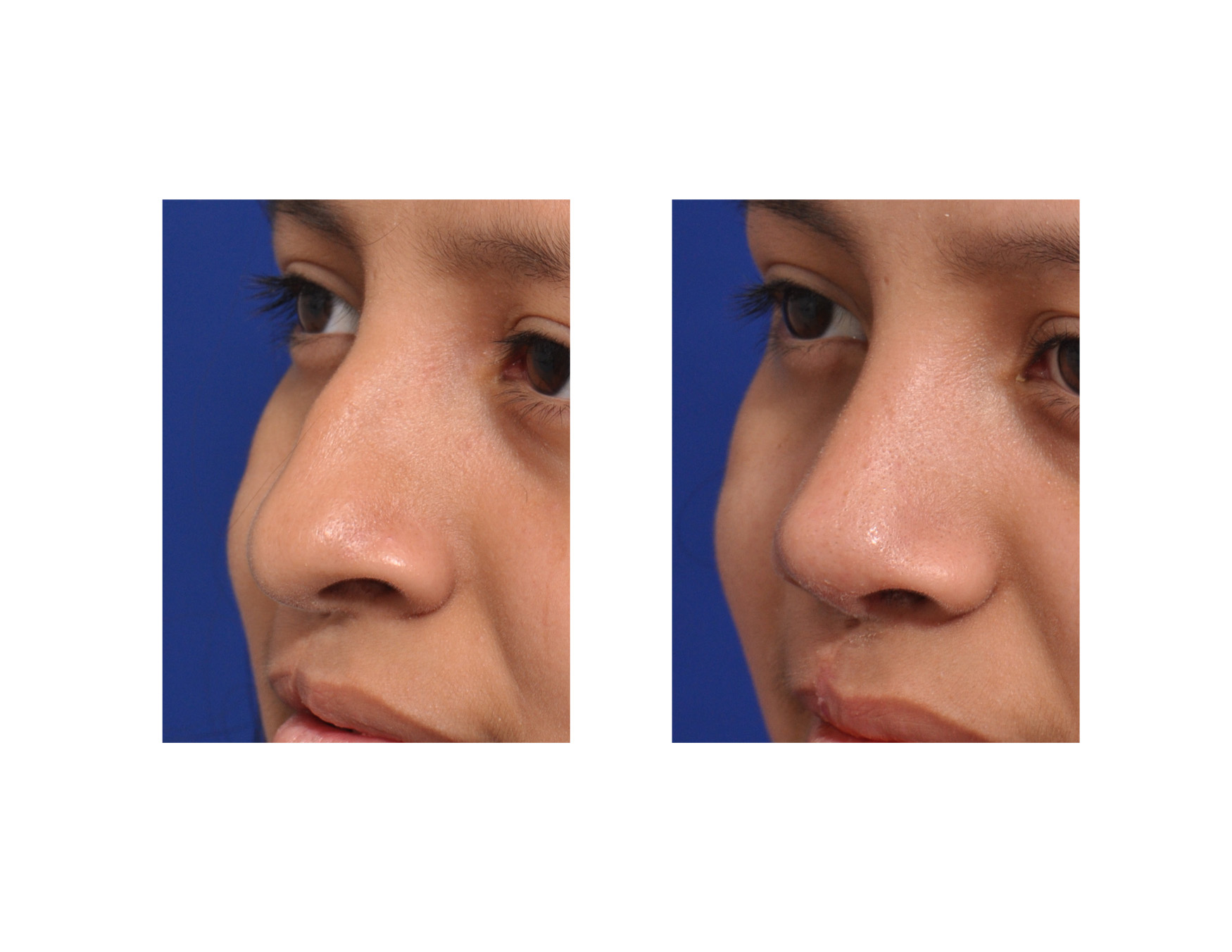 Her six month result shows substantial improvement in the shape of her nose at the tip and nostrils. Lifting of the nasal tip eliminated what appeared to be a prominent nasal hump.Nostril shape and width was improved.
Her six month result shows substantial improvement in the shape of her nose at the tip and nostrils. Lifting of the nasal tip eliminated what appeared to be a prominent nasal hump.Nostril shape and width was improved.
One of the keys to getting improved results in a cleft rhinoplasty is to provide the tip with a strong structural support. The limiting factor is often the size and strength of the cartilage graft. No other graft donor site works as well as that of the rib. It provides a virtually unlimited amount of donor material to be shaped and used as needed. Using the free floating end of rib #9 provides a donor site that can be harvested with a very small incision and minimal recovery.
Highlights:
1) Congenital cleft lip and palate causes a well known set of nasal deformities that affects both sides of the nose.
2) A full open septorhinoplasty is needed to address all the deformities of the cleft nose.
3) Thick nasal skin and a congenital absence of tissue on the cleft side in unilateral cleft lip and palate always limits how much nasal shape improvement can be obtained.
Dr. Barry Eppley
Indianapolis, Indiana