

Background: The brachycephalic skull shape is primarily identified by its effects on the back of the head. A more complete flatness occurs in brachycephaly than in plagiocephaly with the classic very flat and wide back of the head. The increased width may be partially illusionary because of the lack of projection but there is usually a real increased biparietal width that is present.
While the back of the head is the most significantly affected in these type of head shape abnormalities there are frontal effects as well. While the forehead can be somewhat flat as well it is more commonly affected by adverse changes in its slope. Rather than having a more vertical inclination it has a more accentuated backward slope. Lack of forward skull projection is reflected in slope changes rather than lack of just pure horizontal projection that occurs on the back of the head. As a result in brachycephaly one can have a very flat back of the head and a considerable slope of the anterior forehead as well.
In adults all types of skull shape deficiencies, including brachycephaly, are treated by onlay augmentation using custom skull implants. When both the back of the head and forehead are affected a relevant question is whether both can be treated by implant augmentation at the same time.
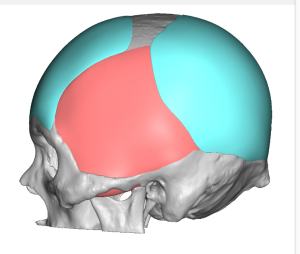
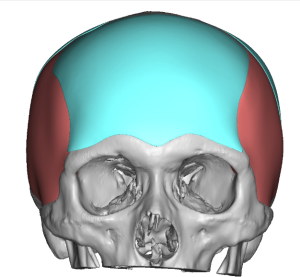
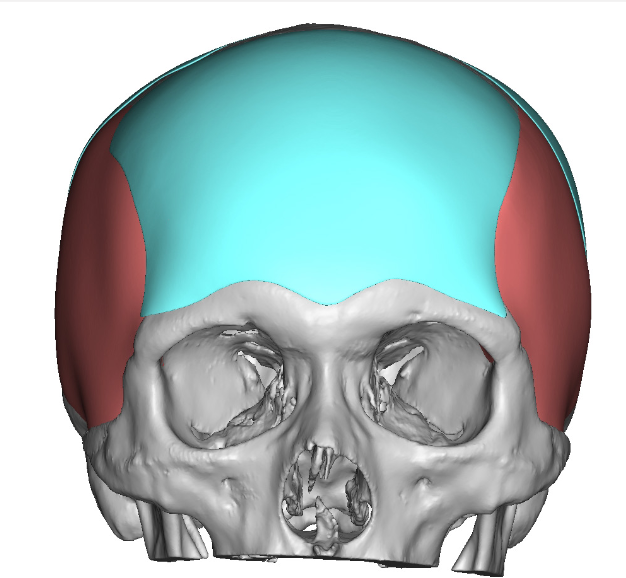
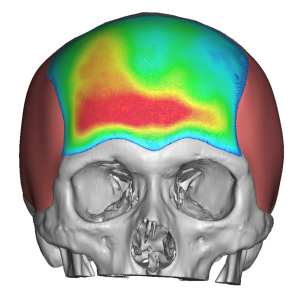 Case Study: This male with a brachycephalic skull shape was planning for a custom skull implant to augment the very flat back of his head. He decided to concurrently do a custom forehead implant as well. This implant was not as thick as that of the back of the head being 5mm maximum projection and 40cc of implant volume. It also corrected some mild asymmetry with the thickest part being on the right side above the brow bone.
Case Study: This male with a brachycephalic skull shape was planning for a custom skull implant to augment the very flat back of his head. He decided to concurrently do a custom forehead implant as well. This implant was not as thick as that of the back of the head being 5mm maximum projection and 40cc of implant volume. It also corrected some mild asymmetry with the thickest part being on the right side above the brow bone.


 After the custom back of the head skull implant has been placed in the prone position under general anesthesia, he was then returned to the supine position for the custom forehead implant. Through a small 3cm scalp incision at the top of the head subperiosteal undermining was done across the entire forehead from one bony temporal line to the other. Dissection was carried down to but not over the brow bones.
After the custom back of the head skull implant has been placed in the prone position under general anesthesia, he was then returned to the supine position for the custom forehead implant. Through a small 3cm scalp incision at the top of the head subperiosteal undermining was done across the entire forehead from one bony temporal line to the other. Dissection was carried down to but not over the brow bones.
 Once the pocket was developed the forehead implant was rolled for insertion and then unrolled once inside the subperiosteal pocket. It was positioned as designed and then secured with two titanium microscrews. Incisional closure was done without the placement of a drain.
Once the pocket was developed the forehead implant was rolled for insertion and then unrolled once inside the subperiosteal pocket. It was positioned as designed and then secured with two titanium microscrews. Incisional closure was done without the placement of a drain.



 His immediate intraoperative result showed the improvement that I would expect from a modestly-sized forehead implant.
His immediate intraoperative result showed the improvement that I would expect from a modestly-sized forehead implant.

 When seen the next day for his head dressing and drain removal the change in his skull length and shape was evident.
When seen the next day for his head dressing and drain removal the change in his skull length and shape was evident.
Both front and back skull implants can be done at the same time providing their volumes are not excessive. As a general rule 150cc implant volume is the limit per skull implantation site if a scalp expansion is not first done. But when the skull implantation sites are completely separate (front and back or side and side) the 150cc volume limit rule can be exceeded as the implantation sites do not intersect or overlap and thus are somewhat independent of each other. I would still be cautious but combined volumes up to 200ccs can be safely done.
Case Highlights:
1) The forehead can be affected in brachycephalic skull shapes with a more backward slope.
2) Custom forehead implants can be design to provide some increased forward projection as well as improve any asymmetries.
3) Custom forehead and back of the head skull implants can be placed during the same surgery using different operative positioning.
Dr. Barry Eppley
Indianapolis, Indiana