

Background: Standard cheek implants have their role in many modest forms of cheek flattening but were never designed to treat a more complete midface deficiency. The more extensive the midface deficiency is the more its effects are seen around the eye. Undereye hollows and pseudoproptosis (bulging off the eye) are the hallmarks of a more complete midface deficiency which extends to involve the lower orbital bones as well.
There are various procedures to augment the lower midface from a LeFort I osteotomy to nasal base-maxillary implants. But when it comes to the upper midface, there are no bone moving procedures that most patients are willing to undergo that would improve the upper maxillary-infraorbital-cheek deficiency. Most patients are not going to undergo a modified LeFort III procedure which would be helpful although still inadequate for an optimal combined infraorbital and cheek augmentation effect.
For the upper midface the only standard implants that are available for augmentation are cheek and tear trough implants. But, as previously mentioned, they were designed for ‘spot’ augmentations for more common aesthetic needs and not to increase a larger area of bony deficiency. The broader and more multidimensional the midface deficiency is the more the need for a custom implant design becomes.

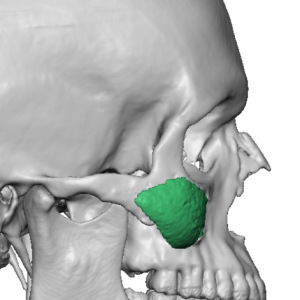
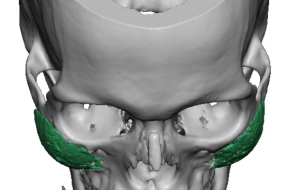 Case Study: This male had a moderates overall midface deficiency which was evident by rounded lower eyelids, pseudoproptosis, upper cheek flatness and nasal base recession. He had a prior history of midface augmentation using standard cheek implants and nasal bone augymentation decades ago, which provided some improvement, but the aesthetic effects were never completely satisfying. His 3D CT scan showed excellent positioning of his silicone malar shell cheek implants of what appeared to be 3 to 4mms of projection.
Case Study: This male had a moderates overall midface deficiency which was evident by rounded lower eyelids, pseudoproptosis, upper cheek flatness and nasal base recession. He had a prior history of midface augmentation using standard cheek implants and nasal bone augymentation decades ago, which provided some improvement, but the aesthetic effects were never completely satisfying. His 3D CT scan showed excellent positioning of his silicone malar shell cheek implants of what appeared to be 3 to 4mms of projection.
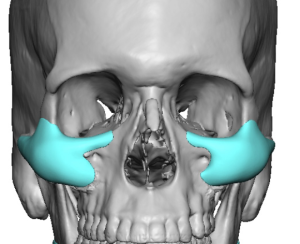
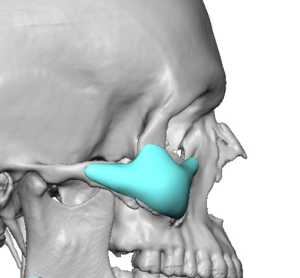
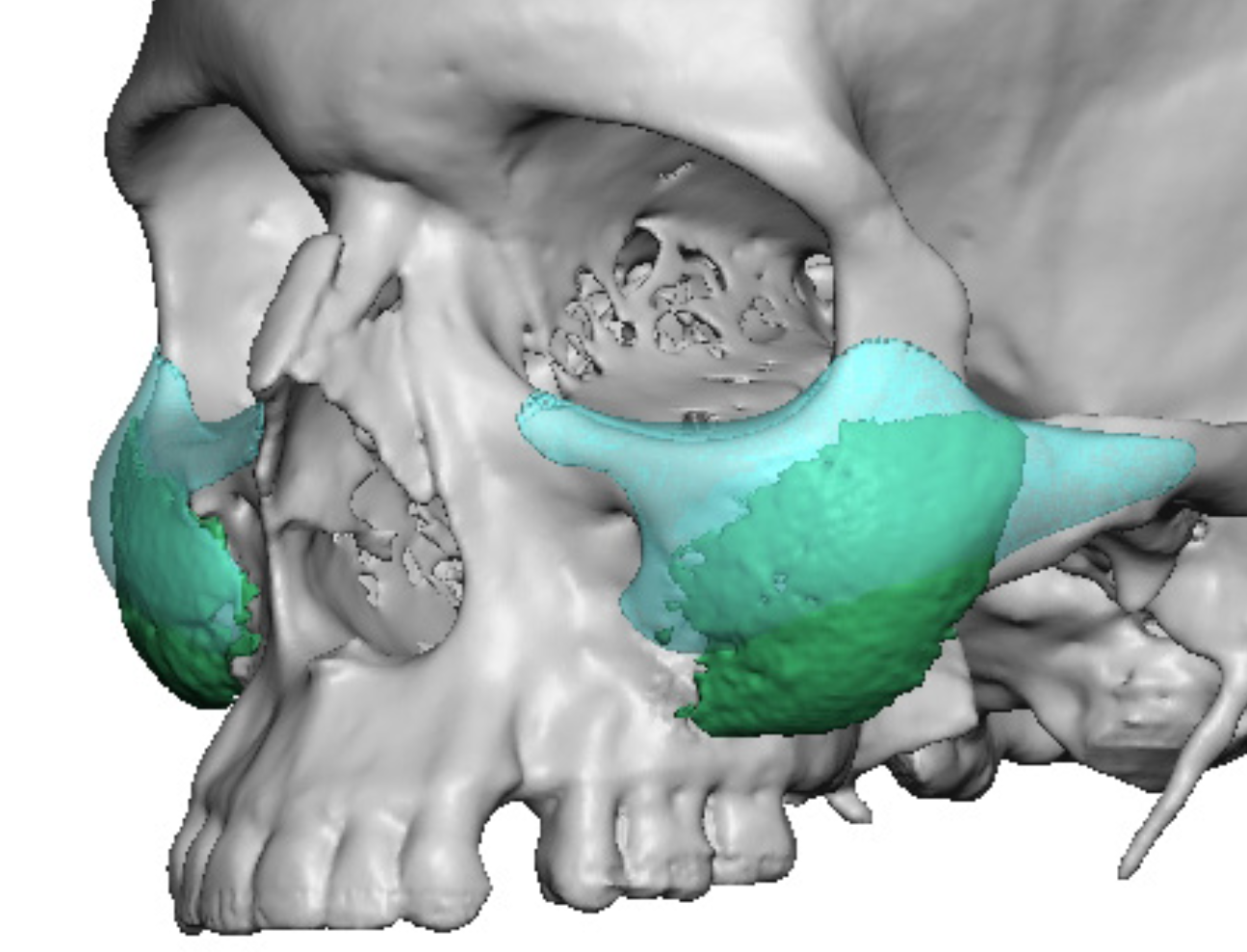
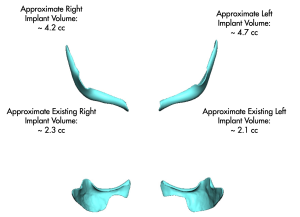
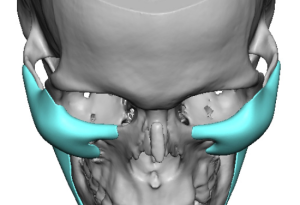 For a more effective midface augmentation effect custom infraorbital-cheek implants were designed whose footprint coverage was complete across the infraorbital rim, part of the lateral orbital rim, and the entire cheekbone down onto the posterior maxillary buttress.
For a more effective midface augmentation effect custom infraorbital-cheek implants were designed whose footprint coverage was complete across the infraorbital rim, part of the lateral orbital rim, and the entire cheekbone down onto the posterior maxillary buttress.
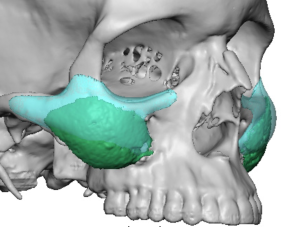
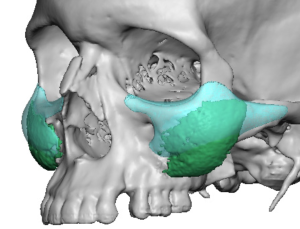 The difference in the surface area coverage of the upper midface could be appreciated when the new design (teal color) was overlaid on the existing cheek implants. (green color)
The difference in the surface area coverage of the upper midface could be appreciated when the new design (teal color) was overlaid on the existing cheek implants. (green color)
 Under general anesthesia and through a lower eyelid incisional approach the upper limits of the indwelling cheek implants could be seen below the infraorbital rim. The cheeks implants were removed and the new implants compared to their custom IOM-cheek replacements.
Under general anesthesia and through a lower eyelid incisional approach the upper limits of the indwelling cheek implants could be seen below the infraorbital rim. The cheeks implants were removed and the new implants compared to their custom IOM-cheek replacements.
With some additional pocket dissection the new custom IOM-cheek implants were placed, which while looking enormous on the outside, did not look that way when implanted.
In fact the midface still looked a bit deficient. So his existing removed cheek implants were modified and placed back as overlays on top of the new custom implants and secured by screws placed through both implants to the bone.
 In a true midface deficiency it can be surprising how much volume of bone is actually ‘missing’. Even when doubling the volume of the design of the new custom IOM-cheek implants with a larger bony surface area, some deficiency still remained in this case. As a result the removed cheek implants were recycled and added on top of the new implants for additional midface volume.
In a true midface deficiency it can be surprising how much volume of bone is actually ‘missing’. Even when doubling the volume of the design of the new custom IOM-cheek implants with a larger bony surface area, some deficiency still remained in this case. As a result the removed cheek implants were recycled and added on top of the new implants for additional midface volume.
Case Highlights:
1) Standard cheek implants are not a good method when mid facial hypoplasia is more complete. (involves the infraorbital rim)
2) Saddling of the infraorbital rim as well as extending along the lateral orbital rim provides augmentation vertically which helps support more horizontal augmentation of the deficient midface.
3) A higher midface augmentation requires a lower eyelid approach for proper implant placement.
Dr. Barry Eppley
Indianapolis, Indiana