

 In the new textbook OPERATIVE TECHNIQUES IN CRANIOFACIAL SURGERY I co-wrote a chapter on craniofacial-based orbital reconstruction entitled ‘Box and U-Shaped Osteotomies’. In this chapter is described the basic techniques for the surgical correction of orbital dystopias. This is a bony orbital condition where the entire orbital box and its contents are displaced in a vertical or horizontal direction from either the normal orbit (unilateral) or from each other. (bilateral)
In the new textbook OPERATIVE TECHNIQUES IN CRANIOFACIAL SURGERY I co-wrote a chapter on craniofacial-based orbital reconstruction entitled ‘Box and U-Shaped Osteotomies’. In this chapter is described the basic techniques for the surgical correction of orbital dystopias. This is a bony orbital condition where the entire orbital box and its contents are displaced in a vertical or horizontal direction from either the normal orbit (unilateral) or from each other. (bilateral)
The most common congenital type of orbital dystopia is hypertelorism. This is where there is an increased interorbital distance and is classified into three types or degrees based on the numerical intercanthal distance. Normal intercanthal distance is around 25 to 28mms, type 1 hypertelorism is 30 to 34mms, type 2 hypertelorism is 34 to 40mms and type 3 hypertelorism is any amount over 40mms. Type 1 hypertelorism is the most common and is non-surgical. It is seen frequently and many people point to Jackie Kennedy/Onassis as an example where it may even be considered attractive. A more contemporary example would be actress Uma Thurman whose facial appearance would be considered both attractive and exotic with her ‘wide set eyes’.
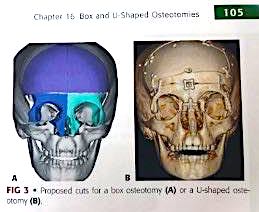
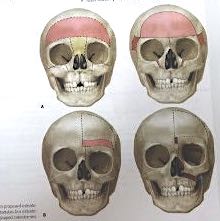 The most common age to treat congenital hypertelorism is between ages 4 to 8 although much older patients can be treated. This is a good age for surgery because the frontal sinuses have not yet developed, the interzygomatic bony distance is nearly adult size and the frontal and orbital bones are still thin enough that osteotomies can be relatively easily performed. Most hypertelorism repair employ a frontal craniotomy or intracranial approach. Box osteotomies can correct both horizontal and vertical dystopias through a 360 degree approach and work best in type 3 hypertelorisms. U-shaped osteotomies, or a 180 degree approach, can be used int type 2 hypertelorisms.
The most common age to treat congenital hypertelorism is between ages 4 to 8 although much older patients can be treated. This is a good age for surgery because the frontal sinuses have not yet developed, the interzygomatic bony distance is nearly adult size and the frontal and orbital bones are still thin enough that osteotomies can be relatively easily performed. Most hypertelorism repair employ a frontal craniotomy or intracranial approach. Box osteotomies can correct both horizontal and vertical dystopias through a 360 degree approach and work best in type 3 hypertelorisms. U-shaped osteotomies, or a 180 degree approach, can be used int type 2 hypertelorisms.
 A contemporary approach for hypertelorism is to use preoperative 3D planning where the bone cuts are performed digitally and intraoperatuve guides provided to help make the bone cuts as well as the new position of the orbital boxes.
A contemporary approach for hypertelorism is to use preoperative 3D planning where the bone cuts are performed digitally and intraoperatuve guides provided to help make the bone cuts as well as the new position of the orbital boxes.
Dr. Barry Eppley
Indianapolis, Indiana