

Background: The size of one’s head or shape of the skull is usually congenitally controlled. While microcephaly is a pathologic skull development condition that restricts brain development, some patients have small narrow heads but not true microcephaly. Sometimes called ‘peanut heads’ and often having issues with wearing hats or helmets their head shape might be called an aesthetic microcephalic condition. It is a normal head size but at the low end of normal.
Aesthetic augmentation of the small head can be done creating a custom total skull implant from the patient’s 3D CT scan. In this design the implant is made to cover the entire head from brow bones to the nuchal ridge in a sagittal dimension and from ear ti ar in a transverse dimension. It does not have to be unduly thick for its effect because of its large surface area coverage. It is very much like simply expanding the entire outer surface of the skull in a circumferential manner.
Unlike skull implants of lesser size, expanding the total outer surface of the skull with an implant requires ensuring that there will be adequate scalp to cover it. One does not want to get caught in surgery and placing the implant and then finding out the incision can not be closed over it. To prevent this very undesirable scenario, it is almost always necessary to first place a tissue expander to initially stretch out the scalp before placing the implant.
Case Study: This young female had long been bothered by the small size of her head. She had narrow sides and a forehead that inclined backward. Her crown height was low and her circumferential skull measurement was in the 15th percentile for an adult female head.
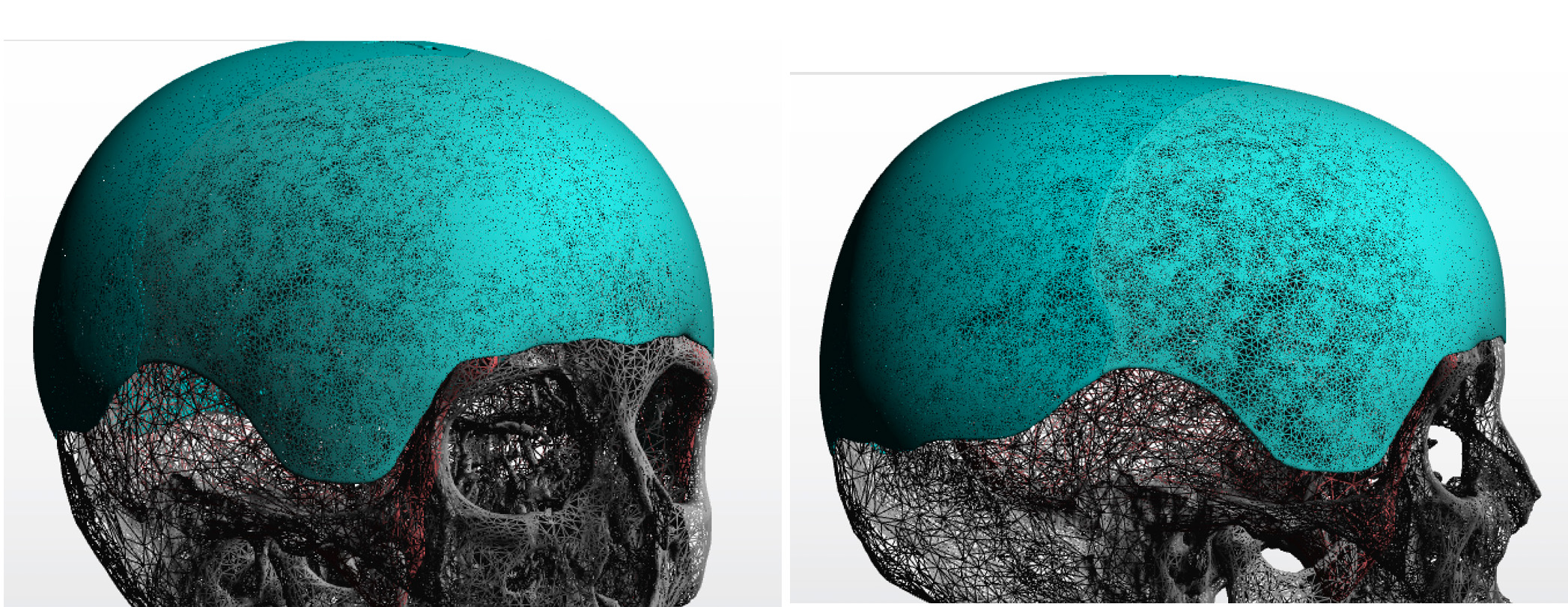
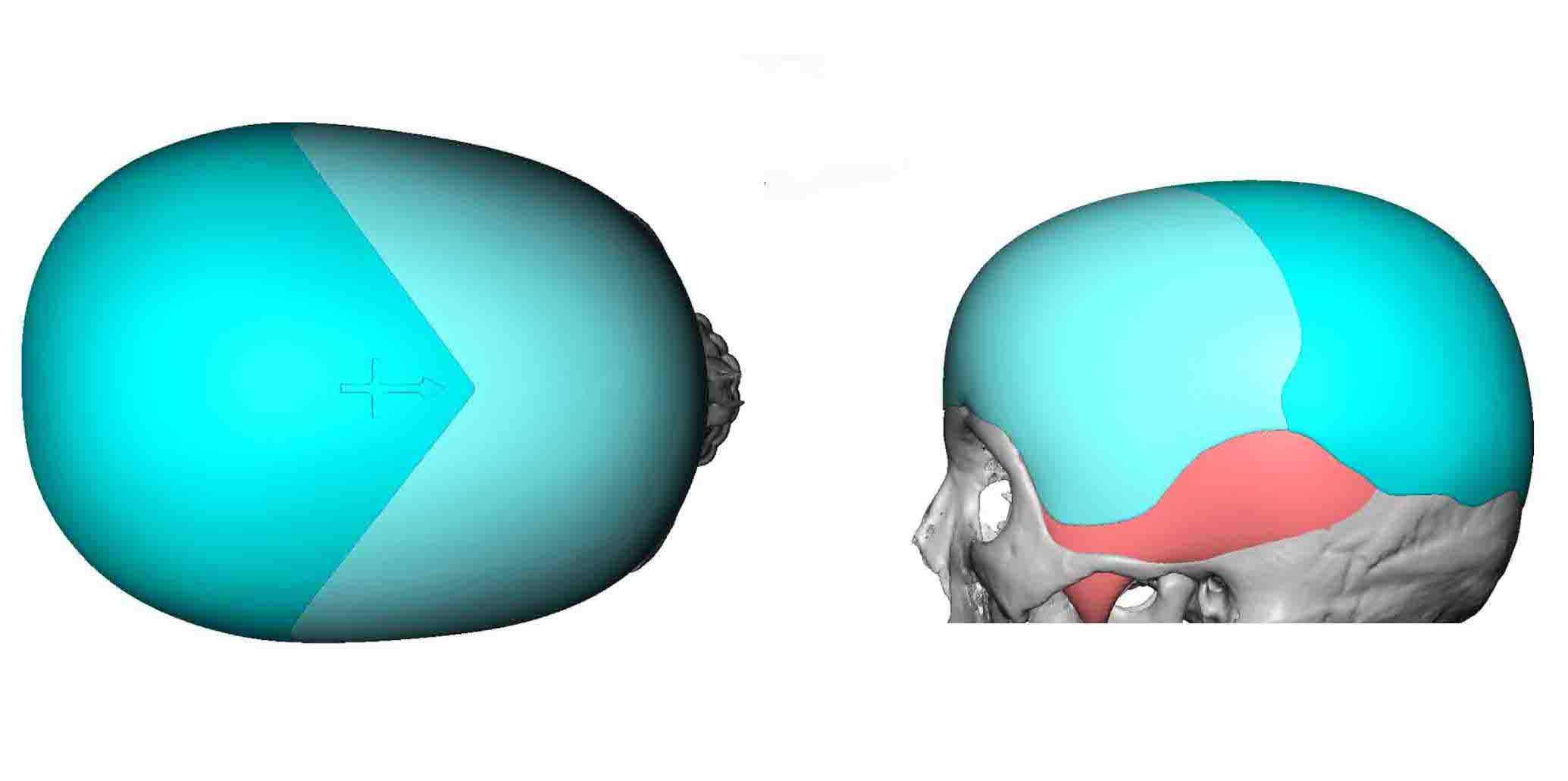 A custom total skull implant was designed that covered her entire bony skull surface including the temporal muscle surface on the sides of her head. Anticipating that the incisional access may not permit such a one-piece implant to be passed into place, a two-piece design was made with an extended V-shaped interface across the top of the implant.
A custom total skull implant was designed that covered her entire bony skull surface including the temporal muscle surface on the sides of her head. Anticipating that the incisional access may not permit such a one-piece implant to be passed into place, a two-piece design was made with an extended V-shaped interface across the top of the implant.
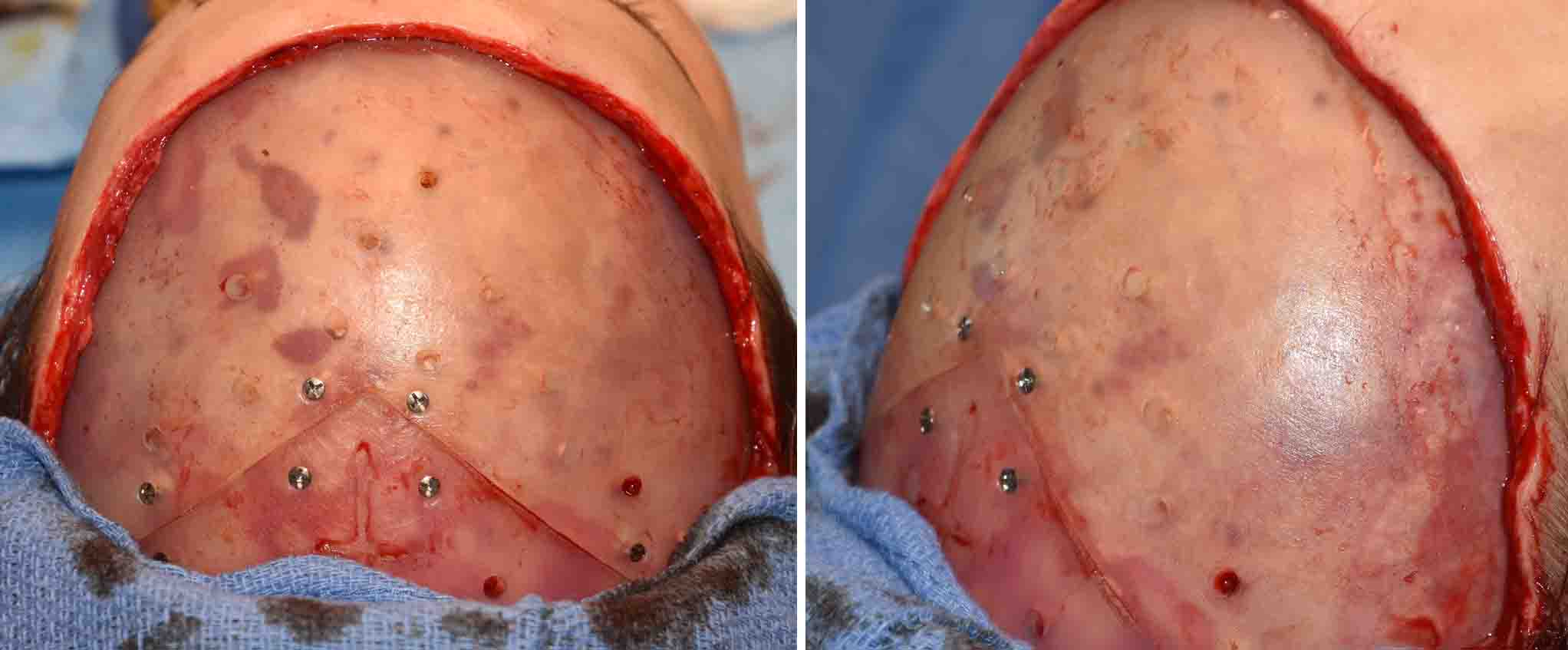 Prior to the placement of the skull implant a scalp expander was placed six weeks previously. It was inflated to 200ccs which was less than the volume of the implant. (226ccs) Due to a prior hairline advancement procedure (another reason for a first stage scalp expansion), the frontal hairline scar was used for incisional access. The tissue expander was removed including all of its capsule. The implant was placed in two pieces and put together after midline alignment and secured on each of the seam with 2.0mm screws. Throughout the implant 4mm perfusion holes were placed. Scalp closure was tight along the frontal hairline but it had a competent closure line.
Prior to the placement of the skull implant a scalp expander was placed six weeks previously. It was inflated to 200ccs which was less than the volume of the implant. (226ccs) Due to a prior hairline advancement procedure (another reason for a first stage scalp expansion), the frontal hairline scar was used for incisional access. The tissue expander was removed including all of its capsule. The implant was placed in two pieces and put together after midline alignment and secured on each of the seam with 2.0mm screws. Throughout the implant 4mm perfusion holes were placed. Scalp closure was tight along the frontal hairline but it had a competent closure line.
A total custom skull implant provides the most significant augmentation to the head that can be done. With a first stage scalp expansion the overall size of the head can be visibly increased. In this case a frontal hairline incision was used. But in patients without a pre-existing scalp scar an incision much further back into the scalp would be used.
Highlights:
1) A custom skull implant can be designed to cover the entire bony and muscular surfaces of the head.
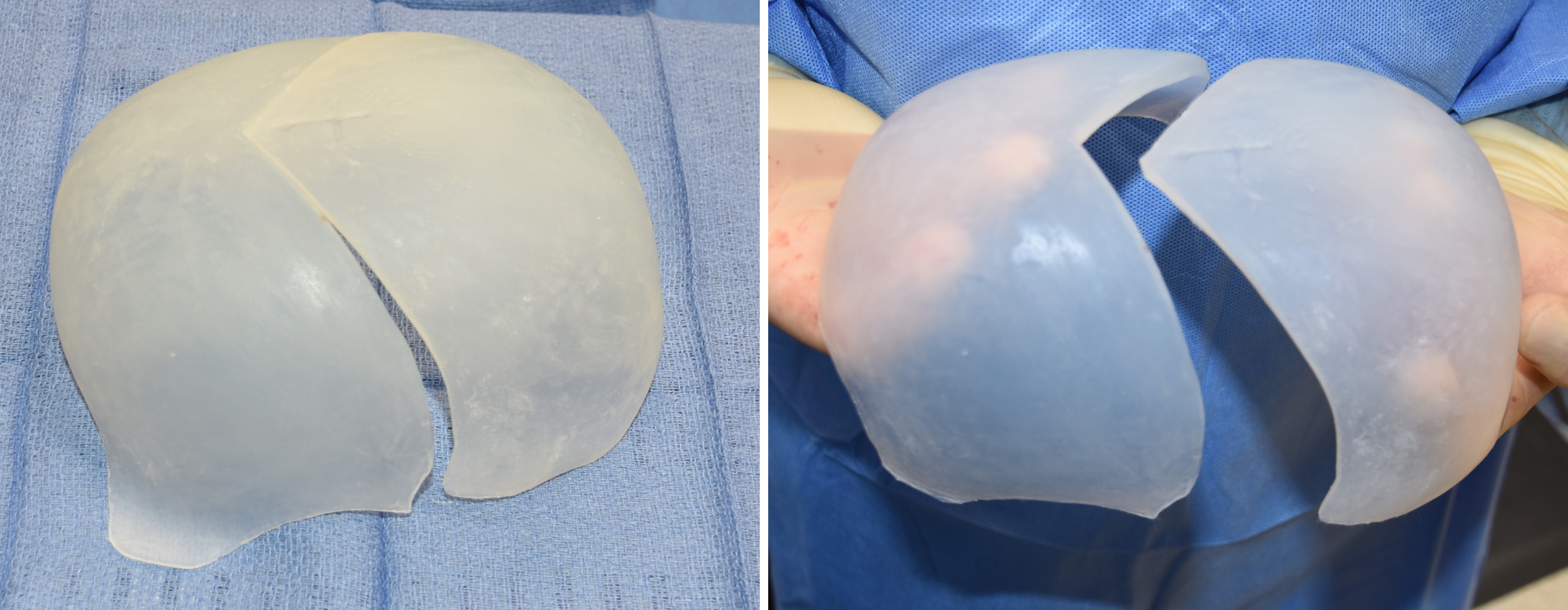
2) Because of covering the entire surface of the skull and the limits of the size of the incision to place it, a custom total skull implant is made in two pieces for insertion and reassembled once in place.
3) A total custom skull implant usually requires a first stage scalp expansion to create adequate scalp closure over the implant.
Dr. Barry Eppley
Indianapolis, Indiana