

Background: The skull, while often perceived as a solid piece of bone, is not. It is actually composed of three layers, very much like an Oreo cookie. There are the outer and inner solid cortical layers (the cookie) and then there is a thinner inner layer which is softer known as the diploid or marrow space. (the filling)
Many skull defects occur as a result of injuries caused by fractures of varying degrees of the bone’s thickness. When the skull fracture does not significantly displace the inner cortical table and does not disrupt the dura, there is no need for surgical reduction. But such fractures often do displace the outer cortical table resulting in contour defects. The soft tissue will eventually follow the depressed bone inward as scar contracture and healing ensure.
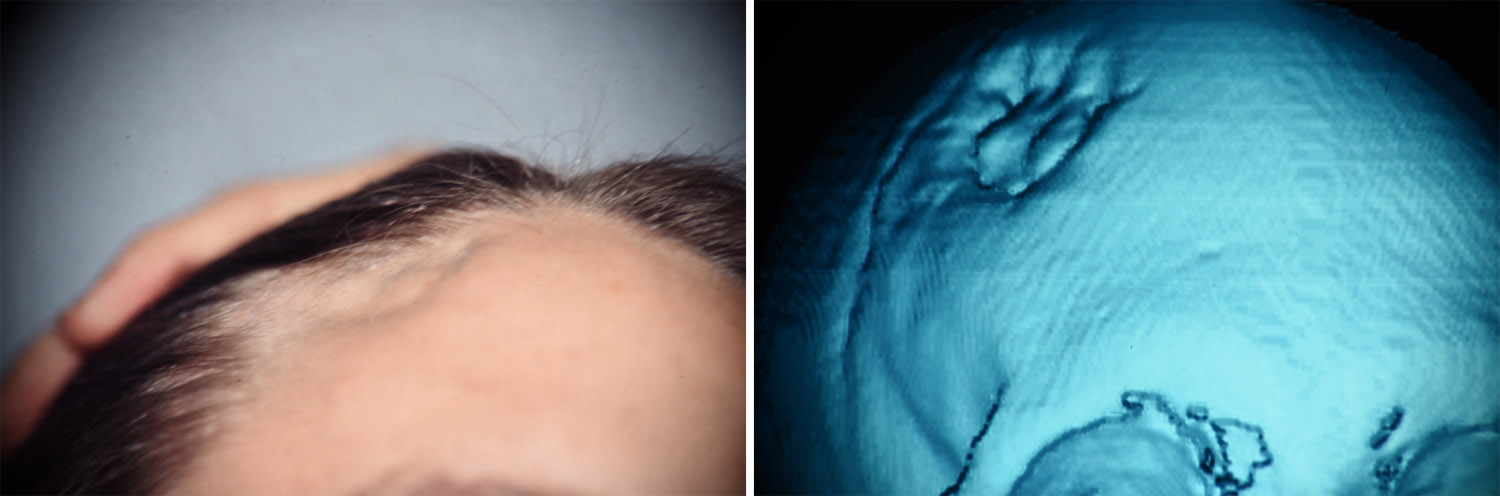 Case Study: This 24 year-old male was involved in a car accident in which he sustained blunt trauma to his right upper forehead. He sustained a full thickness skull fracture with a small underlying epidural bleed. He was not treated surgically and he went on to a full recovery. As he healed he developed a circular indentation over the fracture site. A 3D CT scan showed that it was due to a bone indentation caused by his previous skull fracture.
Case Study: This 24 year-old male was involved in a car accident in which he sustained blunt trauma to his right upper forehead. He sustained a full thickness skull fracture with a small underlying epidural bleed. He was not treated surgically and he went on to a full recovery. As he healed he developed a circular indentation over the fracture site. A 3D CT scan showed that it was due to a bone indentation caused by his previous skull fracture.
 Under general anesthesia, a semicircular hairline incision was made for access and the defect exposed. The fractured bone was stable and no effort was made to elevate the fracture segments. The defect was filled with hydroxyapatite granules and covered with a 1m thick resorbable plate with screws for containment.
Under general anesthesia, a semicircular hairline incision was made for access and the defect exposed. The fractured bone was stable and no effort was made to elevate the fracture segments. The defect was filled with hydroxyapatite granules and covered with a 1m thick resorbable plate with screws for containment.

 His after surgery result showed the restoration of a smooth external forehead/skull contour.
His after surgery result showed the restoration of a smooth external forehead/skull contour.
The use of hydroxyapatite bone substitute today in skull reconstruction, and for almost the past twenty years now, has been with using it in a bone cement form. This provides the best method of application as it is contoured into the defect site and then sets before wound closure. But hydroxyapatite can be still used in granular form which allows for true fibrovascular ingrowth and even some bone ingrowth as well. Its use is restricted to a completely contained skull defect with an underlying floor and walls.
Highlights:
- Small skull defects can be treated by a wide variety of cranioplasty materials.
- In a small partial-thickness skull defect, hydroxyapatite granules can be used to fill the defect and create a smooth cranial contour.
- A resorbable cover can be used as a roof for a hydroxyapatite granule skull reconstruction.
Dr. Barry Eppley
Indianapolis, Indiana