

Jaw reduction is a generic term for different types of lower facial reshaping procedures. Often lumped into one general category, the reality is that a variety of bone and muscle reduction procedures are available to create a lower face that appears more narrow or slimmer. Each jaw reduction procedure differs in the specific dimensional changes that are created in the lower face. The two general types of jaw reductions can target either muscle and bone.
Masseter Muscle Reduction

 The masseter muscle is a large soft tissue structure that is stretched out between the zygomatic arch (origin) and the bony jaw angle. (insertion)When the masseter muscle is overly enlarged due to natural congenital size or hypertrophied due to over activity (e.g., chronic clenching) it can create a wide looking lower jaw. It can be treated non-surgically by Botox injections. (or Dysport or Xeomin) This works by causing a reduction in the size of the muscle fibers which reduces the thickness of the muscle. The injections are localized to the part of the muscle over the bony jaw angle below the ear which is coincidentally the safest place for injection therapy to avoid buccal branches of the facial nerve which lie above it. The effect of the muscle reduction is usually seen by about three weeks after an injection treatment and will last about 3 months when the size of the muscle slowly returns. In some patients with enough Botox treatments the reduction in the size of the masseter muscles may be more long lasting or even permanent but this is the exception and does not commonly occur.
The masseter muscle is a large soft tissue structure that is stretched out between the zygomatic arch (origin) and the bony jaw angle. (insertion)When the masseter muscle is overly enlarged due to natural congenital size or hypertrophied due to over activity (e.g., chronic clenching) it can create a wide looking lower jaw. It can be treated non-surgically by Botox injections. (or Dysport or Xeomin) This works by causing a reduction in the size of the muscle fibers which reduces the thickness of the muscle. The injections are localized to the part of the muscle over the bony jaw angle below the ear which is coincidentally the safest place for injection therapy to avoid buccal branches of the facial nerve which lie above it. The effect of the muscle reduction is usually seen by about three weeks after an injection treatment and will last about 3 months when the size of the muscle slowly returns. In some patients with enough Botox treatments the reduction in the size of the masseter muscles may be more long lasting or even permanent but this is the exception and does not commonly occur.
Surgical masseter muscle reduction can also be done but this does not refer to the excision of segments of the muscle. This is generally not a preferred technique of muscle reduction due to the risks of intraoperaive bleeding and the high likelihood of creating external contour irregularities. An alternative approach which is similar to radiofrequency ablation is electocautery reduction. With this technique an incision is made inside the mouth and the inner surface of the muscle is lifted off of the bone. The inner surface of the muscle is then treated by direct electrocautery using a fine tipped needle at spot locations in a grid pattern. This has no risks of causing bleeding or muscle irregularities. The thermal injury to the muscle all cause it to partially shrink over time whose reduction will be permanent due to loss of muscle fibers.
Bony Jaw Reduction
Jaw Angle Reduction


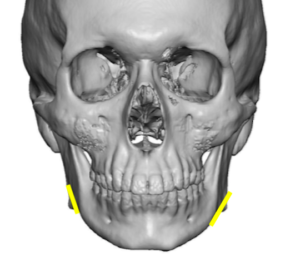 While the chin is the leading corner of the lower jaw, the jaw angles are the paired back corners. Like the chin they can be similarly reduced although their dimensional changes are less complex when done in isolation. Reducing their width or flare makes the appearance of the jawline slimmer from the front view and creates a facial shape this less wide or square. By reducing their width but not the vertical length the shape of the jaw angle is preserved and there is little risk of soft tissue sag due to loss of bony support. This is typically done through an intraoral approach by a bone burring technique to remove the outer layer of bone and jaw angle point. It can also be done more directly from an external skin incision in the neck if one wants to completely avoid the recovery from an intraoral approach.
While the chin is the leading corner of the lower jaw, the jaw angles are the paired back corners. Like the chin they can be similarly reduced although their dimensional changes are less complex when done in isolation. Reducing their width or flare makes the appearance of the jawline slimmer from the front view and creates a facial shape this less wide or square. By reducing their width but not the vertical length the shape of the jaw angle is preserved and there is little risk of soft tissue sag due to loss of bony support. This is typically done through an intraoral approach by a bone burring technique to remove the outer layer of bone and jaw angle point. It can also be done more directly from an external skin incision in the neck if one wants to completely avoid the recovery from an intraoral approach.
V Line Jaw Reduction
The term ‘v line surgery’ refers to a complete or total jaw reduction procedure that reduces the bone from the jaw angles in the back to the chin in the front. It can be a confusing term because it technically has several variations which differ based on the specific dimensions of the jaw that need to be reduced. Jaw bone removal can be done either in a partial thickness (shaving or lateral corticotomies) or full thickness excision. (ostectomies)
 For patients with very wide and/or a vertically long lower jaw, a full-thickness of bone is removed in a curved fashion from the jaw angles to the chin. This changes the complete shape of the bone not only in width but in length as well. (changes the mandibular plane angle) It produces the most dramatic amount of jaw reduction but also risks over-resection when applied to the wrong type of jaw shape. This is what is done in traditional v-line surgery. It is no surprise that this type of jaw reduction emanates from Asia where the natural shape of the lower jaw is more square and needs full thickness excisions for a significant shape change and a more noticeable narrowing effect.
For patients with very wide and/or a vertically long lower jaw, a full-thickness of bone is removed in a curved fashion from the jaw angles to the chin. This changes the complete shape of the bone not only in width but in length as well. (changes the mandibular plane angle) It produces the most dramatic amount of jaw reduction but also risks over-resection when applied to the wrong type of jaw shape. This is what is done in traditional v-line surgery. It is no surprise that this type of jaw reduction emanates from Asia where the natural shape of the lower jaw is more square and needs full thickness excisions for a significant shape change and a more noticeable narrowing effect.

 While less well known V line surgery can also be done by shaving or by removing the outer layer of bone which changes the width of the jaw but not its vertical length. The jaw angle shape is kept intact but it becomes less wide. The amount of jaw reduction change is less dramatic but is more aesthetically appropriate for jaw shapes that are not unduly wide or flared and don’t have a low jaw angle. It is often what is better suited for the patient who has a normal mandibular plane angle and has little risk of resulting in an over resected lower jaw shape. When combined with chin narrowing/lengthening the v line effect is enhanced.
While less well known V line surgery can also be done by shaving or by removing the outer layer of bone which changes the width of the jaw but not its vertical length. The jaw angle shape is kept intact but it becomes less wide. The amount of jaw reduction change is less dramatic but is more aesthetically appropriate for jaw shapes that are not unduly wide or flared and don’t have a low jaw angle. It is often what is better suited for the patient who has a normal mandibular plane angle and has little risk of resulting in an over resected lower jaw shape. When combined with chin narrowing/lengthening the v line effect is enhanced.
The key to a successful bony jaw reduction is to match the technique with the dimensional requirements needed for the desired change. This not only requires preoperative x-rays (panorex, lateral cephalogram or 3D jaw CT scan) but computer imaging to determine what magnitude of jaw reduction change the patient desires. While under- and over resection results can occur, by far the most common revisional jaw reduction patients I see is when too much has been done. This almost always is when traditional v-line surgery has left the patient with over resected jaw angles and chin that is too narrow or elongated. This can be a function of overly aggressive bone reduction but more commonly occurs because it was not the right technique for the patient’s natural jaw shape.
Dr. Barry Eppley
Indianapolis, Indiana