


Background: Treatment of the overly wide or convex head shape requires a temporal reduction procedure. The side of the head is known as the temporal region which has a large muscle component external to the thinner temporal bone underneath. It iswell known in temporal craniotomies for brain tumors and aneurysms that loss of temporal muscle fullness results in significant temporal hollowing. Such knowledge has been applied to aesthetic head width narrowing through temporal muscle removal…which has a less severe and more aesthetically pleasing outcome.
While many believe that it requires temporal bone removal to cause a head narrowing effect such an approach is ineffective and causes undue scarring. Assessment of many CT scans show that the temporal muscle thickness just above the ear is as thick if not thicker than the underlying bone. Even though it is a masticatory muscle partial removal of it has no negative effects on jaw movement.
There are two techniques in temporal reduction for head narrowing, subtotal (posterior) muscle excision and muscle transposition. Understanding their differences is based on the somewhat arbitrary separation of the temporal muscle into an anterior and posterior part. The temporal muscle is really one continuous muscle but the anterior part (by the side of the eye and in front of the ear) is thicker and overlies the very concave temporal fossa bone. The posterior part is above the ear and extends to the back of the head, it is thinner and overlies the slightly convex part of the temporal bone. The subtotal excision technique works well when the head width is caused by a fuller posterior region alone. The muscle transposition technique is indicated when both the anterior region along with the posterior region is the source of the excessive width.
Regardless of the temporal reduction technique used once the muscle is removed the parietal eminence or tuberosity area of the skull may become more exposed and stick out like a point at the top side of the posterior skull. Many times the prominent parietal eminence is recognized by the patient before temporal reduction surgery and this area of skull reduction should be incorporated into the surgery.
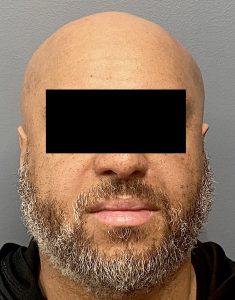
 Case Study: This male was bothered by the wide round shape of his head as evidenced by anterior and posterior temporal fullness. He was also aware of a prominent parietal tuberosity which he could see in the oblique view of his head. The surgical plan consisted of temporal muscle transposition with bony parietal eminence reduction for a total side of the head narrowing.
Case Study: This male was bothered by the wide round shape of his head as evidenced by anterior and posterior temporal fullness. He was also aware of a prominent parietal tuberosity which he could see in the oblique view of his head. The surgical plan consisted of temporal muscle transposition with bony parietal eminence reduction for a total side of the head narrowing.

 Under general anesthesia postauricular incisions were made and dissection carried down to the deep temporal fascia. The temporal muscle was widely released from the bone on its underside as well as released from the overlying fascia on its outer side. This release was also carried along the origin of the muscle along the bony temporal line.
Under general anesthesia postauricular incisions were made and dissection carried down to the deep temporal fascia. The temporal muscle was widely released from the bone on its underside as well as released from the overlying fascia on its outer side. This release was also carried along the origin of the muscle along the bony temporal line.
![]() The temporal muscle was then rotated down and back and partial delivered the out through the incision. The now excessive muscle was trimmed and sutured down to a fascial cuff made during the initial fascial incision. This effectively rotates the temporal muscle down and back, reducing both anterior and posterior areas.
The temporal muscle was then rotated down and back and partial delivered the out through the incision. The now excessive muscle was trimmed and sutured down to a fascial cuff made during the initial fascial incision. This effectively rotates the temporal muscle down and back, reducing both anterior and posterior areas.

 Lastly through the same incision a large #8 skull rasp was used to reduce the bone 2 to 3mms over the parietal eminence on both sides.
Lastly through the same incision a large #8 skull rasp was used to reduce the bone 2 to 3mms over the parietal eminence on both sides.

 A layered closure using resorbable sutures was then done over a drain.
A layered closure using resorbable sutures was then done over a drain.
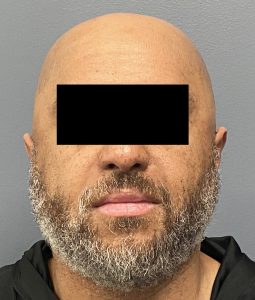 His one day post operative result immediately after his head dressing and drain removals showed a more straight side of the profile even with swelling present. This will eventually turn into a more square head shape in the front view as the swelling resolves over the next 4 to 6 weeks.
His one day post operative result immediately after his head dressing and drain removals showed a more straight side of the profile even with swelling present. This will eventually turn into a more square head shape in the front view as the swelling resolves over the next 4 to 6 weeks.
Case Highlights:
1) Temporal muscle reduction is the most effective method of narrowing a wide head.
2) Of the two types of temporal reduction surgery for head width narrowing the muscle transposition technique creates a reduction in both the anterior and posterior muscle zones.
3) In any form of temporal reduction bony parietal eminence reduction may be needed to reduce the posterior-superior high spot at the back end of the muscle.
Dr. Barry Eppley
World-Renowned Plastic Surgeon