


Background: The length of the head is the distance from the frontal bone of the forehead to the occipital bone on the back of the head. When increased anteroposterior head lengths occur there is always an increased occipital length component. With that occipital protrusion comes a change in the shape of the back of the head from a modest convexity to more of a parabolic curve shape.
In these congenital head shapes, which are very ethnically-based, the increased occipital projection (often referred to as an occipital bun) has both an extra- and intracranial component to it. The occipital bone is always thicker but 100% of the protrusion is not bone alone. There is an extension of the occipital lobe of the brain as well. Thus in bony reductions of an occipital bun a completely normalization of the back of the head shape may not be possible.
Occipital bun reductions are like most any other skull reduction the outer table of the skull bone is removed, stopping just shy of the very vascular diploic space. The question is never whether any skull reduction can be done but how much is safely achievable and whether that amount of reduction is worth the effort. Tracing over a lateral skull x-ray along with computer imaging can help the patient make that preoperative determination.
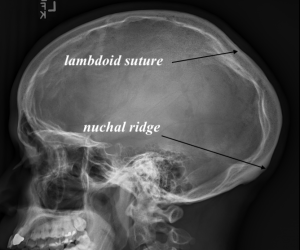
 Case Study: This male had a large protrusion on the back of his head that created an unnatural convex shape. A lateral skull film showed the amount of bone protrusion and thickness as well as the location of the brain. (Intracranial surface)
Case Study: This male had a large protrusion on the back of his head that created an unnatural convex shape. A lateral skull film showed the amount of bone protrusion and thickness as well as the location of the brain. (Intracranial surface)
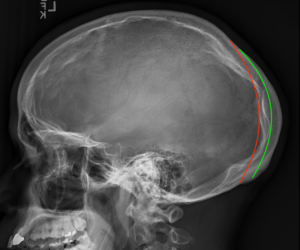 The x-ray also shows the relevant anatomic landmarks for an occipital bone reduction procedure as well as how much of a reduction can be safely accomplished. (green line = amount of safe bone reduction, red line = amount of bone removal needed for a completely normal back of head shape)
The x-ray also shows the relevant anatomic landmarks for an occipital bone reduction procedure as well as how much of a reduction can be safely accomplished. (green line = amount of safe bone reduction, red line = amount of bone removal needed for a completely normal back of head shape)

 Under general anesthesia and in the prone position a low horizontal scalp incision was made and the entire occipital bone exposed by subperiosteal elevation. Using a high speed and a 6mm carbide round burr radiating cut lines were done in the bone from the incision creating a sunray pattern of bone lines up to the lambdoid suture lines. The bone cuts were right down to but not into the diploic space. The occipital bone was removed between these cut lines and a smooth lowered surface was created.
Under general anesthesia and in the prone position a low horizontal scalp incision was made and the entire occipital bone exposed by subperiosteal elevation. Using a high speed and a 6mm carbide round burr radiating cut lines were done in the bone from the incision creating a sunray pattern of bone lines up to the lambdoid suture lines. The bone cuts were right down to but not into the diploic space. The occipital bone was removed between these cut lines and a smooth lowered surface was created.
 Once the bone was removed a drain was placed and a two layer scalp closure was done using resorbable sutures.
Once the bone was removed a drain was placed and a two layer scalp closure was done using resorbable sutures.

 When the head dressing and the drain was removed the next day the change in the protrusion could be seen in profile.
When the head dressing and the drain was removed the next day the change in the protrusion could be seen in profile.
In the occipital bun in a congenitally elongated head shape significant bone reduction can be done and a visible improvement in head shape seen. But it is imp0rtant to check a preoperative x-ray to determine how much bone can be removed as well as where is the inner cranial surface is compared to the amount of bone reduction possible. Such radiographic analysis will usually sh0w that a completely normal back of the head shape is not achievable although visible reduction in the protrusion is.
Key Points:
1) Most protrusions on the back on the head are due to overgrowth of the occipital bone below the lambdoid sutures.
2) A preoperative x-ray confirms that the protrusion on the back of the head has a significant bone thickness to it that is safely reducible.
3) Occipital bony reductions are done using a radiating cortical cut pattern done through a low scalp incision over the nuchal ridge.
Dr. Barry Eppley
World-Renowned Plastic Surgeon