

Background: Plagiocephaly is a unique form of craniofacial asymmetry and its probably the best known because of its syndromic presentation from its axial twisting developmental pattern. With predominant symptom of a flat back of the head on one side (right more frequently than left), which is often the major issue, there is a series of associated craniofacial asymmetries that can occur with it depending on the extent of the deformity. When describing these associated craniofacial asymmetries the basis is the flat back of the head side and every other affected area is described from it as either being on the same side (ipsilateral) or the opposite side. (contralateral)
The most common associated symptoms to the flat back of the head are anterior facial manifestations with ipsilateral facial protrusions of the ear and the right facial skeleton. Less commonly seen are contralateral back of the head protrusions opposite the flat side and contralateral facial skeletal deficiencies.
The flat back of the head is the most frequently requested area of correction in adult plagiocephaly as it is the most severely affected. This is typically done using custom skull implant designs which wrap around onto the posterior temporal region. Facial corrections can be done concurrently and the decision has to be made whether to reduce the overprotecting side or augment the flatter contralateral side. While the diagnosis is technically a facial protrusion in the ipsilateral side it is far easier to augment the ‘normal’ side than it is to reduce the overprojected side.
One of the more uncommon manifestations of plagiocephaly is that the opposite side of the back of the head sticks out too far. This often extends further into the side of the head making it having excessive width as well. When this exists augmentation of the flat side of the back of head will provide an improvement but not a complete correction.
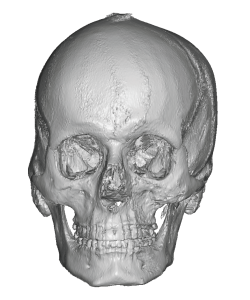
 Case Study: This male had significant craniofacial asymmetry that had the following components which were bothersome to him; 1) a flat right back of the head that extended all the way to the side of the forehead, 2) a contralateral left back of the head protrusion that extended into the temporal region, 3) a left infraorbital-maxillary recession and 4) a left jawline deficiency. His only other prior surgery to treat any of these asymmetries was an intraoral left zygomatic expansion osteotomy. (which did improve cheek width but not projection)
Case Study: This male had significant craniofacial asymmetry that had the following components which were bothersome to him; 1) a flat right back of the head that extended all the way to the side of the forehead, 2) a contralateral left back of the head protrusion that extended into the temporal region, 3) a left infraorbital-maxillary recession and 4) a left jawline deficiency. His only other prior surgery to treat any of these asymmetries was an intraoral left zygomatic expansion osteotomy. (which did improve cheek width but not projection)
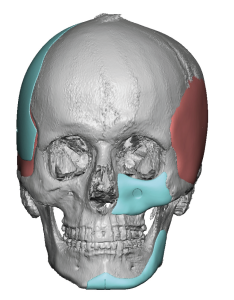
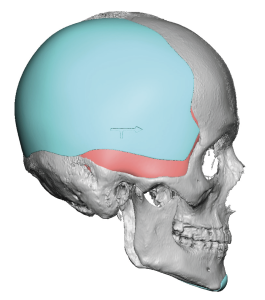
 A comprehensive treatment plan to treat all of his most bothersome craniogfacial asymmetries consisted of: 1) a right back of the head custom implant that augmented the entire right side of this head up to the side of his forehead, 2) a custom left infraorbital-maxillary implant, 3) a left custom jawline implant, 4) left temporal muscle reduction by muscle removal, and 5) a left parietal eminence skull reduction to treat the bulging.
A comprehensive treatment plan to treat all of his most bothersome craniogfacial asymmetries consisted of: 1) a right back of the head custom implant that augmented the entire right side of this head up to the side of his forehead, 2) a custom left infraorbital-maxillary implant, 3) a left custom jawline implant, 4) left temporal muscle reduction by muscle removal, and 5) a left parietal eminence skull reduction to treat the bulging.



 The first step in his craniofacial asymmetry surgery was the placement of the large right custom back of head-temporal implant. This was done through a three incision technique, a postauricular incision behind the ear and two very small anterior and posterior scalp incision. Through these incisions a subperiosteal pocket was made over the occipital-parietal bone and extended on top of the deep temporal fascia to the side of the forehead. The implant was introduced from behind the ear and once positioned a screw was placed through the two small scalp incisions for fixation. A drain was placed and all incisions closed with resorbable sutures.
The first step in his craniofacial asymmetry surgery was the placement of the large right custom back of head-temporal implant. This was done through a three incision technique, a postauricular incision behind the ear and two very small anterior and posterior scalp incision. Through these incisions a subperiosteal pocket was made over the occipital-parietal bone and extended on top of the deep temporal fascia to the side of the forehead. The implant was introduced from behind the ear and once positioned a screw was placed through the two small scalp incisions for fixation. A drain was placed and all incisions closed with resorbable sutures.

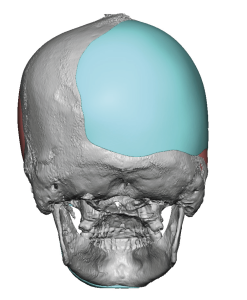
 The next step was a left temporal muscle reduction from a postauricular incision combined with rasping down of the more remote parietal eminence from the same incision.
The next step was a left temporal muscle reduction from a postauricular incision combined with rasping down of the more remote parietal eminence from the same incision.
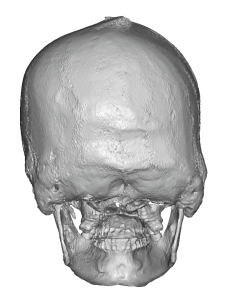
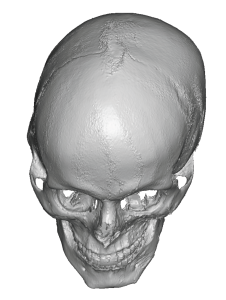
 From a skull reshaping standpoint much better symmetry was seen in the front view of the two sides of the head.
From a skull reshaping standpoint much better symmetry was seen in the front view of the two sides of the head.


 The left facial augmentations were completed by the placement of the left custom jawline implant through a combined submental skin and intraoral posterior vestibular incisions. Screw fixation was done at the chin anteriorly and the jaw angle posteriorly.
The left facial augmentations were completed by the placement of the left custom jawline implant through a combined submental skin and intraoral posterior vestibular incisions. Screw fixation was done at the chin anteriorly and the jaw angle posteriorly.
Lastly the left custom infraorbital-maxillary implant was placed through an intraoral incision from his prior left zygomatic osteotomy.
 Craniofacial asymmetry surgeries are often a combination of augmentation of deficient areas and reduction of prominent ones. The augmentation aspect produces more significant changes than reduction as more volume can always be added than what can be reduced. With custom implants designs skull and facial deficiencies can be simultaneously treated to maximize the surgical effort. When looking at a more complete craniofacial asymmetry correction as in this case the task can seem daunting but taking it one section at a time allows for an overall changes that was completed in 3 1/2 hours.
Craniofacial asymmetry surgeries are often a combination of augmentation of deficient areas and reduction of prominent ones. The augmentation aspect produces more significant changes than reduction as more volume can always be added than what can be reduced. With custom implants designs skull and facial deficiencies can be simultaneously treated to maximize the surgical effort. When looking at a more complete craniofacial asymmetry correction as in this case the task can seem daunting but taking it one section at a time allows for an overall changes that was completed in 3 1/2 hours.
Case Highlights:
1) Plagiocephaly can cause a total craniofacial asymmetry that affects the contralateral facial side from that of the back.
2) In some flat back of the head plagiocephalys the opposite side of the flat back of the head becomes too prominent and must be factored into the skull correction.
3) The contralateral facial flatness can be built out using custom implant designs to complete a total craniofacial asymmetry correction.
Dr. Barry Eppley
Indianapolis, Indiana