

Background: One of the most common and recognized non-synostotic skull deformities is that of plagiocephaly. Technically this is a generic descriptive term that refers to a flat spot on the head, particularly in babies and children. But it is most commonly seen as a flat area on the back of the head when viewed from above. The ear is almost always noted to be pushed forward on the flatter side.
While in some patients the occipital flattening may be self-correcting and early helmet therapy is the standard treatment to do in the first several years of life, when seen in adults it is a surgically treatable problem only. While the facial effects caused by plagiocephaly may pose their own aesthetic issues in either males or females, adult males are most consistently bothered by the occipital flattening. The obvious reason is shorter hair, thinning hair, or a shaved/bald head.
The effects of plagiocephaly are always more severe on the back of the head than on the face. This speaks to the origin of plagiocephaly which is from the deformational forces that occur during development or after birth. Its correction in adults focuses on the cosmetic overlay or augmentation of the deficient side of the back of the head.
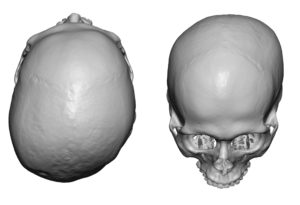 Case Study: This young male adult had a significant plagiocephaly with moderately severe flattening of the right side of his head. The ipsilateral ear was further forward than the opposite ear and had a greater outer protrusion. The forehead, cheek and brow bone was also slightly more further forward as well.
Case Study: This young male adult had a significant plagiocephaly with moderately severe flattening of the right side of his head. The ipsilateral ear was further forward than the opposite ear and had a greater outer protrusion. The forehead, cheek and brow bone was also slightly more further forward as well.
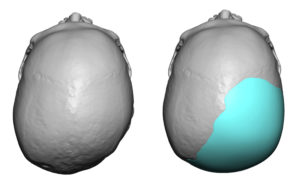
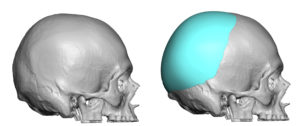
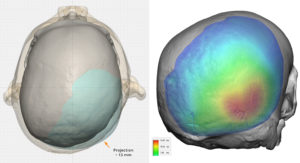 A custom skull implant was designed for the back of the head to match the contours of the left side of the back of the head. This combined occipital-parietal skull implant needed to cover all of the right occiput and most of the parietal bone. The total volume of the implant was 103ccs.
A custom skull implant was designed for the back of the head to match the contours of the left side of the back of the head. This combined occipital-parietal skull implant needed to cover all of the right occiput and most of the parietal bone. The total volume of the implant was 103ccs.

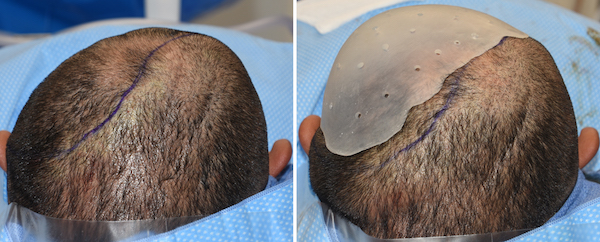
 Under general anesthesia and in the prone position a 3D printed plastic mold of the implant was initially tried on to see how it fit. This allowed an outline of its position to be marked on the scalp.
Under general anesthesia and in the prone position a 3D printed plastic mold of the implant was initially tried on to see how it fit. This allowed an outline of its position to be marked on the scalp.


 Thereafter a low 7 cm long horizontal scalp incision was made over the midline of the occiput about 3 cms above the inion. The subperosteal pocket was developed and the implant prepared by placing perfusion holes in it. The implant was inserted using a rolled technique and positioned using the compass marker visible through the incision. The key was to release enough scalp inferiorly to ensure that the implant sat low enough on the skull. Once in good position two screws were used on each side of the midline for positional stability.
Thereafter a low 7 cm long horizontal scalp incision was made over the midline of the occiput about 3 cms above the inion. The subperosteal pocket was developed and the implant prepared by placing perfusion holes in it. The implant was inserted using a rolled technique and positioned using the compass marker visible through the incision. The key was to release enough scalp inferiorly to ensure that the implant sat low enough on the skull. Once in good position two screws were used on each side of the midline for positional stability.
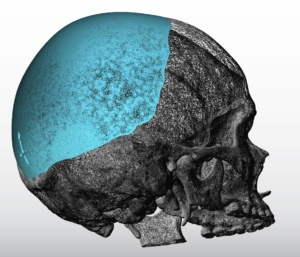
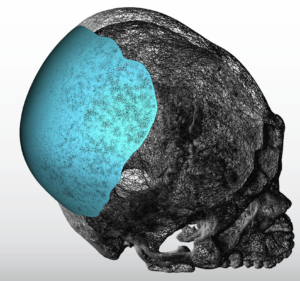 In looking at the extent of a plagiocephaly skull deformity, it is important to recognize how much of the parietal bone is involved. Technically all of it is and this is actually more of a parietal skull deformity than an occipital one by surface area. Getting the custom skull implant to ‘turn the corner’ sufficiently and come forward to cover the parietal bone on top and at the side is the key to maximize the augmentation effect that is needed. Recognizing that the ear is pushed forward speaks to the anterior extent along the parietal bone and even into the posterior temporal bone that is involved.
In looking at the extent of a plagiocephaly skull deformity, it is important to recognize how much of the parietal bone is involved. Technically all of it is and this is actually more of a parietal skull deformity than an occipital one by surface area. Getting the custom skull implant to ‘turn the corner’ sufficiently and come forward to cover the parietal bone on top and at the side is the key to maximize the augmentation effect that is needed. Recognizing that the ear is pushed forward speaks to the anterior extent along the parietal bone and even into the posterior temporal bone that is involved.
Case Highlights:
1) Plagiocephaly is most commonly seen as a flatness of one side of the back of the head although its effects are seen throughout the entire skull.
2) Augmentation of the flat occipital area is best done with a custom designed skull implant.
3) Because of the extent of many plagiocephalic skull deformities the surface area coverage of the custom skull implant is greater than one may think in the parietal bone area.
Dr. Barry Eppley
Indianapolis, Indiana