


Background: Skull implants represent a new type of aesthetic augmentation procedure in the ability to reshape one’s head. Just like any other face or body feature, however, there are gender specific types of changes that apply to the head as well. While women’s head shapes are overall smaller as would be expected, their bone thicknesses are actually very similar. In general it is the raised areas of the skull in which gender differences occur such as the brow bones, temporal lines and the inion and nuchal ridges on the back of the head. Such topographic features are more prominent in men.
Aesthetically one feature that appears to be a preference for women over men is in the crown area. The crown is located at the upper back of the head and is really the junction of the top and back of the skull. It is a curved semi-circular area that largely is composed of the parietal bone. From a scalp nomenclature standpoint it is known as the vertex. Increased height in this area is desired by women and is an almost an exclusive gender specific request. When men refer to increased projection on the back of their head they usually mean a straight back increase. But women usually mean increased crown projection. That is as critical understanding when designing skull implants for men vs women.
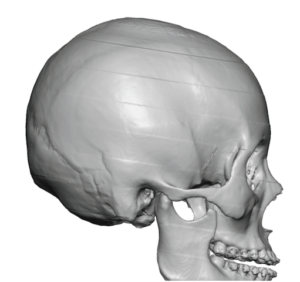
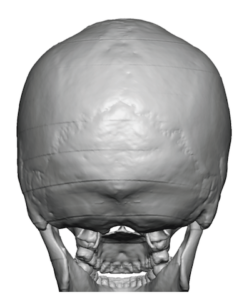 Case Study: This female was bothered by lack of projection on the back of her head with emphasis on the crown area. Interestingly her 3D CT scan showed parasagittal grooving as it extended forward from the crown area….a sequelae of a flat posterior parietal area that I have seen many times before.
Case Study: This female was bothered by lack of projection on the back of her head with emphasis on the crown area. Interestingly her 3D CT scan showed parasagittal grooving as it extended forward from the crown area….a sequelae of a flat posterior parietal area that I have seen many times before.
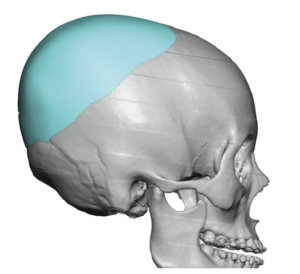
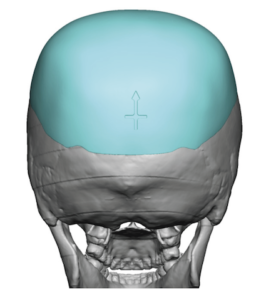
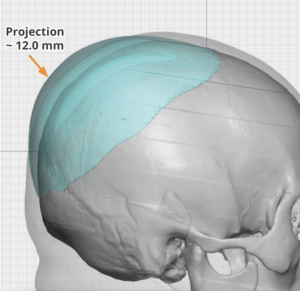
 Her custom skull implant design had a footprint that extended forward to cover the parasagittal grooving as well as far enough along the sides to look natural. The maximim projection point was in the crown area of 12mmms with a total implant volume of 160ccs.
Her custom skull implant design had a footprint that extended forward to cover the parasagittal grooving as well as far enough along the sides to look natural. The maximim projection point was in the crown area of 12mmms with a total implant volume of 160ccs.


 Under general anesthesia in the prone position the skull implant was placed through an irregular zigzag scalp incision located on the back of the head of 9 cms length. Getting such a large skull implant in placed through an aesthetically small incision requites a combination of implant design (inner grooves), material durometer and technical expertise in intrapocket implant positioning.
Under general anesthesia in the prone position the skull implant was placed through an irregular zigzag scalp incision located on the back of the head of 9 cms length. Getting such a large skull implant in placed through an aesthetically small incision requites a combination of implant design (inner grooves), material durometer and technical expertise in intrapocket implant positioning.
Two of the major factors to consider in any skull implant design is: 1) volume based on the ability of the scalp to stretch to accommodate it, and 2) being able to get the implant in through the desired length of the scalp incision. There is no exact science to it, it is one learned by a lot of experience. But as a general rule custom skull implant can generally be inserted and tolerated if the initial implant volume is around the 150cc range, +/- 10cc based on the thickness of the patient’s scalp.
Case Highlights:
1) Female skull implants typically focus on the maximum point of augmentation in the crown area.
2) The crown of the skull is whether the scalp is the tightest as the intersection between the top and back of the head which must be considered in both implant volume and surface areas coverage.
3) Getting skull implants through small scalp incisions is a function of their flexibility and creation of the implant pocket.
Dr. Barry Eppley
Indianapolis, Indiana