


Background: The greatest aesthetic head shape deficiency in females is on its posterior surface or the back of the head. While commonly referred to as the occiput this is anatomically inaccurate. The back of the head is composed of multiple skull bones of which the singular occipital bone makes up only the lower half. The upper half of the back of the head is made up of the paired parietal bones. Together these 3 bones make up the total back of the head and their development and union give it its shape.
But this anatomic makeup may seem merely descriptive it has relevance in understanding the patient’s head shape concerns and how to design an implant to properly augment it. A true or completely flat back of the head involves the parietal and occipital bones while a crown/upper back of the head deficiency is more limited to the parietal bones. This understanding allows for the angulation of maximal projection to be determined for the implant design.
In the horizontal back of head deficiency the point of maximal projection is located more over the midline of the parietal-occipital junction. But in crown skull deficiencies the point of maximal projection moves superiorly onto the parietal bone completely. As a result the footprint of the implant shifts where it sits on the skull, keeping the point of projection centrally located on the implant.
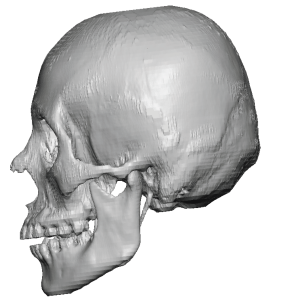 Case Study: This female desired augmentation of a congenital flat back of head in which a 3D CT scan showed a lack of convexity starting above the nuchal ridge of the occipital bone.
Case Study: This female desired augmentation of a congenital flat back of head in which a 3D CT scan showed a lack of convexity starting above the nuchal ridge of the occipital bone.
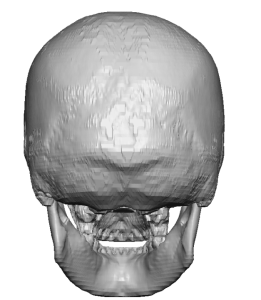
 In addition there was a distinct midline groove in the parietal bone which extended down into the occipital bone. This was clearly a sagittal suture indentation.
In addition there was a distinct midline groove in the parietal bone which extended down into the occipital bone. This was clearly a sagittal suture indentation.
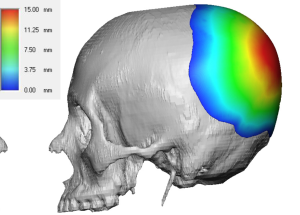
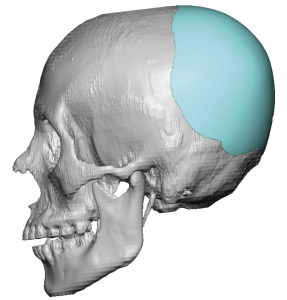 Using the same scan a custom skull implant was designed for the back of the head with a maximum projection of 15mms centered over the parietal-occipital junction for an almost completely horizontal augmentation effect.. The total implant volume was 145ccs.
Using the same scan a custom skull implant was designed for the back of the head with a maximum projection of 15mms centered over the parietal-occipital junction for an almost completely horizontal augmentation effect.. The total implant volume was 145ccs.

 Under general anesthesia and in the prone position the custom skull implant was placed through a horizontal scalp incision centered above the nuchal ridge. But before its placement the implant was prepared by the placement of multiple 5mm perfusion holes. Once inserted it was secured with small microscrews. The scalp incision was closed over a drain.
Under general anesthesia and in the prone position the custom skull implant was placed through a horizontal scalp incision centered above the nuchal ridge. But before its placement the implant was prepared by the placement of multiple 5mm perfusion holes. Once inserted it was secured with small microscrews. The scalp incision was closed over a drain.

 When seen the next day for head dressing and drain removal the improvement in her back of the head shape could be seen.
When seen the next day for head dressing and drain removal the improvement in her back of the head shape could be seen.
Key Points:
1) For females the most common type of skull augmentation is for the flat back of the head or deficient crown area.
2) The pure horizontal back the head implant design has its point of maximal projection located on or near the sagittal-lambdoid suture junction.
3) For most female patients the maximal implant size (volume) is 150ccs but will be lower in thinner scalps.
Dr. Barry Eppley
World-Renowned Plastic Surgeon