

Background: Jaw asymmetries are one of the most common congenital facial asymmetries that present in a wide range of expressions. Most are small type asymmetries that most people would barely notice. But the more significant ones are more obvious with chins that are shifted to one side and with jaw angles that are profoundly different in shape from the front view.
In the more significant jaw asymmetries orthognathic surgery plays a major role in their correction. Realigning the lower jaw in a more midline position with a sagittal split osteotomy (with or without an upper LeFort osteotomy) helps center the chin and improve the lower jaw appearance. But on the shorter side of the jaw asymmetry (the side where the chin was deviated to) the smaller jaw angle will remain asymmetric in appearance. A sagittal split, as its name implies, creates a sagittal movement of the jaw and can do little for any width issues at the osteotomy site. (ramus) Often the smaller jaw angle becomes more asymmetric in appearance as the rest of the lower jaw becomes centrically aligned.
It is tempting in jaw angle asymmetries to believe that taking any form of a standard implant (or some intraoperative modification thereof) will produce an adequate correction. What is more likely to happen is that just a different type of jaw asymmetry will remain. It is very difficult by external appearance to judge the missing dimensions of the jaw angle bone.

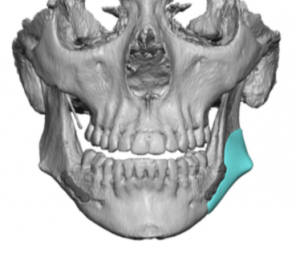
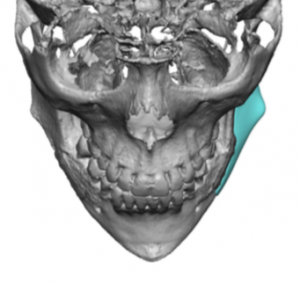
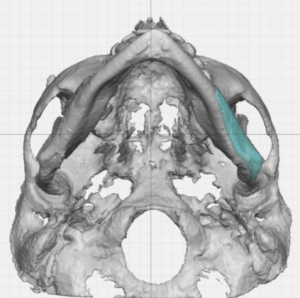
 Case Study: This female had a congenital jaw asymmetry which was initially treated by sagittal split osteotomies. This adequately aligned her chin with a pleasing right jaw angle shape but the left jaw angle remained significantly different in appearance. A 3D CT scan shows the extent of the left jaw angle bony asymmetry.
Case Study: This female had a congenital jaw asymmetry which was initially treated by sagittal split osteotomies. This adequately aligned her chin with a pleasing right jaw angle shape but the left jaw angle remained significantly different in appearance. A 3D CT scan shows the extent of the left jaw angle bony asymmetry.
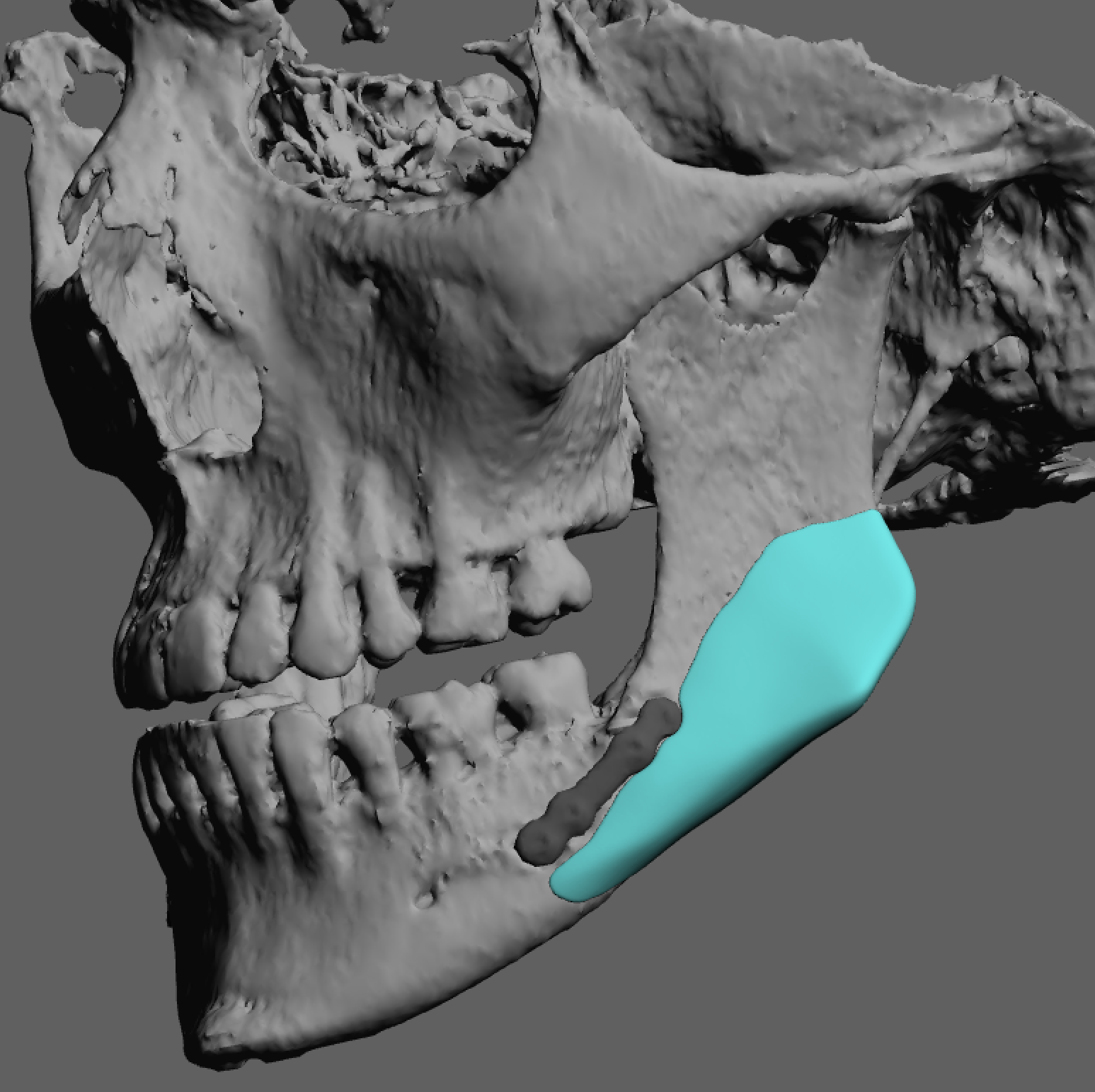
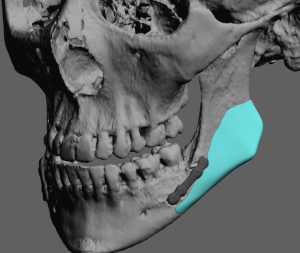
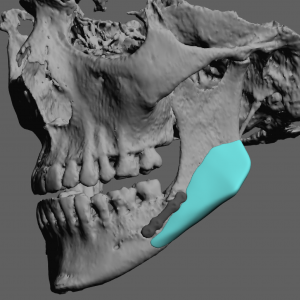
 Using the 3D CT scan a left jaw angle implant was designed using a mirroring technique. She had an usually sharp or pointy type jaw angle shape which is not common in females.
Using the 3D CT scan a left jaw angle implant was designed using a mirroring technique. She had an usually sharp or pointy type jaw angle shape which is not common in females.
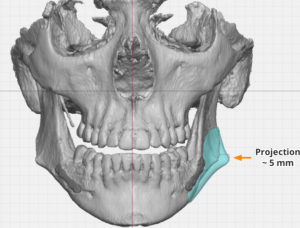
 Besides the shape the dimensions of the implant were very specific with 5mms of width at the widest part of the jaw angle projection.
Besides the shape the dimensions of the implant were very specific with 5mms of width at the widest part of the jaw angle projection.

 Under general anesthesia and through a posterior integral vestibular incision lateral to her prior sagittal split incision, a subperiosteal pocket was developed elevating the masseter muscle off the bone. To get the implant in its designed position the ligamentous attachments of the muscle needed to be released from bone around the jaw angle point. The custom jaw angle implant with preplanned screws as inserted and positioned. Using a transcutaneous screwdriver the implant was secured to the bone.
Under general anesthesia and through a posterior integral vestibular incision lateral to her prior sagittal split incision, a subperiosteal pocket was developed elevating the masseter muscle off the bone. To get the implant in its designed position the ligamentous attachments of the muscle needed to be released from bone around the jaw angle point. The custom jaw angle implant with preplanned screws as inserted and positioned. Using a transcutaneous screwdriver the implant was secured to the bone.
 The anatomy of the bony jaw angle is highly specific to each patient. While often seen as a simple bone shape, as almost all standard jaw angle implants would imply, is not accurate. While the coverage of the thick masseter muscles does camouflage some of the jaw angle bone shape, the thinnest part of the muscle is over the most prominent part of it. For these reasons a custom designed jaw angle shape offers the best chance for optimal asymmetry correction in the back part of the lower jaw.
The anatomy of the bony jaw angle is highly specific to each patient. While often seen as a simple bone shape, as almost all standard jaw angle implants would imply, is not accurate. While the coverage of the thick masseter muscles does camouflage some of the jaw angle bone shape, the thinnest part of the muscle is over the most prominent part of it. For these reasons a custom designed jaw angle shape offers the best chance for optimal asymmetry correction in the back part of the lower jaw.
Case Highlights:
1) Orthognathic surgery improves the sagittal chin position and the occlusion but usually fails to correct width and vertical asymmetries of the jaw angles.
2) Jaw angle asymmetries are more optimally improved by custom implant designs than the use of a standard implant.
3) Many custom jaw angle implants for asymmetries are smaller and with more complex shapes than one would think and require precise placement in the toughest area to implant in the face to be effective.
Dr. Barry Eppley
Indianapolis, Indiana