

Background: The occipital bone is the most posterior projection of the skull. It is a curved bone of which only its upper half is seen externally. Its lower half extends inferiorly beneath the thick neck muscles and provides the aperture for the spinal column. The upper half of the occipital bone has a superior border with the lambdoidal suture line which is significant in occipital bone protrusions or the occipital bun deformity. When the occipital bone grows excessively there is a distinct takeoff or step-off from the lambdoid suture line onto the occipital bone.
The question in occipital protrusions is whether this is due to excessive bone thickness or is it a protrusion from the push of the underlying brain with the overlying bone having normal thickness. (or is even thinner than normal) This becomes critical to know if a reduction is being planned as that question will determine whether an aesthetically visible reduction can be achieved. While in many patients the occipital bun is due to an increased bone thickness a plain lateral skull film or a 2D non-contrast scan will provide the definitive answer.
The occipital bone, like all other seven cranial bones, has a three layer composition with an outer and inner solid table of bone between which lies the thin diploic space. (cancellous bone) The occipital bone is the thickest of all the cranial bones particularly at its ridges and protuberances. This bodes favorably for a significant reduction which is done by removal of the outer table of bone down close to the diplopia space.
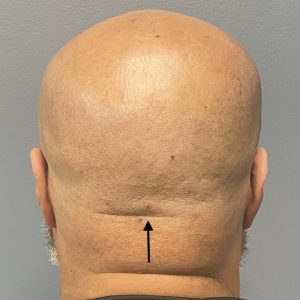 Case Study: This young male was bothered by a prominent bulge on the back of his head. By physical examination the occipital bone can be felt raised up superiorly along the lambdoidal suture line. Preoperative imaging was done to show the patient the type of change I felt could be achieved by its reduction…which the patient felt was acceptable. He had a convenient high neck incision which could be used for the incision location.
Case Study: This young male was bothered by a prominent bulge on the back of his head. By physical examination the occipital bone can be felt raised up superiorly along the lambdoidal suture line. Preoperative imaging was done to show the patient the type of change I felt could be achieved by its reduction…which the patient felt was acceptable. He had a convenient high neck incision which could be used for the incision location.

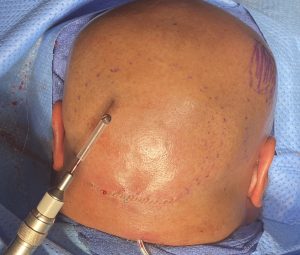 Under general anesthesia and in the prone position the horizontal neck wrinkle line was used for the incision which was just over the bottom end of the nuchal ridge. The key to the occipital bone reduction is the length of the burr on the high speed handpiece. Because of the length of the incision the burr can be introduced further up into the subperiosteal pocket than then bottom end of the burr…but not by a large amount. This is why the incision can not be very low or in a horizontal neck incision that is below the bottom end of the nuchal ridge by any significant distance. The entire outer cortical bone layer of the occipital bone is removed in a curved fashion… rounding out the sides to prevent creating a flat spot. Closure is done over a drain with a two layer resorbable suture closure.
Under general anesthesia and in the prone position the horizontal neck wrinkle line was used for the incision which was just over the bottom end of the nuchal ridge. The key to the occipital bone reduction is the length of the burr on the high speed handpiece. Because of the length of the incision the burr can be introduced further up into the subperiosteal pocket than then bottom end of the burr…but not by a large amount. This is why the incision can not be very low or in a horizontal neck incision that is below the bottom end of the nuchal ridge by any significant distance. The entire outer cortical bone layer of the occipital bone is removed in a curved fashion… rounding out the sides to prevent creating a flat spot. Closure is done over a drain with a two layer resorbable suture closure.

 He had a good intraoperative reduction in the shape of the back of his head with the outer cortical bone removal.
He had a good intraoperative reduction in the shape of the back of his head with the outer cortical bone removal.

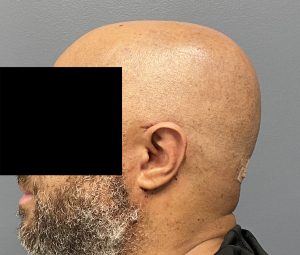 His one day post operative result immediately after his head dressing and drain removal showed the elimination of his back of the head protrusion.
His one day post operative result immediately after his head dressing and drain removal showed the elimination of his back of the head protrusion.
Case Highlights:
1) Occipital bone enlargement is one of the most common skull reduction areas requested by men.
2) The usual approach to occipital skull reduction is a horizontal incision in a high neck skin crease.
3) A guarded high speed bone burring technique is used to remove the outer cortical bone layer down next to the diploic space.
Dr. Barry Eppley
World-Renowned Plastic Surgeon