

Background: A softer face in a male is always associated with less strong and angular facial bone development. The facial bones may be in good balance and not have any obvious disharmony. But stronger bony prominences are lacking. This is most noteworthy at the corners of the face which I define as the chin and jaw angles on the lower face and the cheeks in the midface.
 With these gender defining points comes the linear or arched connections between them. For the cheeks this includes the infraorbital rims and the zygomatic arches. Thus with less prominent cheeks comes weaker infraorbital rims and increased infraorbital hollows and lack of any visible zygomatic arches. For the jawline the body between the chin and jaw angles lacks width and may have a more inward curvature making it indistinct.
With these gender defining points comes the linear or arched connections between them. For the cheeks this includes the infraorbital rims and the zygomatic arches. Thus with less prominent cheeks comes weaker infraorbital rims and increased infraorbital hollows and lack of any visible zygomatic arches. For the jawline the body between the chin and jaw angles lacks width and may have a more inward curvature making it indistinct.
The most comprehensive method to change the prominences and shape of these midfacial and jawline structures is with custom implants. While many perceive that such implants are used to create dramatic changes, they are just as effective at smaller magnitudes of change. And for many men who may be smaller in body stature, more discrete forms of custom cheek and jawline implants are better suited to their aesthetic needs and will prevent them from looking unnatural or having too dramatic a facial change.
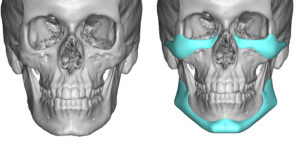
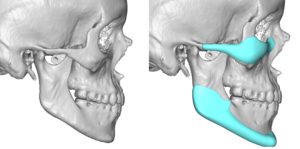 Case Study: This younger male presented for a facial masculinizing change. He wanted a somewhat stronger jawline and more prominent cheeks as well as to improve his infraorbital hollows. Using his 3D CT scan custom infraorbital-malar and jawline implants were designed with sizes that would be described in my experience as modest to moderate.
Case Study: This younger male presented for a facial masculinizing change. He wanted a somewhat stronger jawline and more prominent cheeks as well as to improve his infraorbital hollows. Using his 3D CT scan custom infraorbital-malar and jawline implants were designed with sizes that would be described in my experience as modest to moderate.
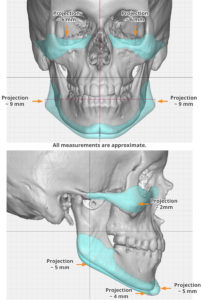 Such measurements as 5mm horizontal chin projection, 9mms jaw angle width and 2mms cheek projection are examples of modest to average linear facial augmentations. What these modest implant sizes do is primarily create some angularity/convexity at the important facial bony areas as well as more pronounced connections between them
Such measurements as 5mm horizontal chin projection, 9mms jaw angle width and 2mms cheek projection are examples of modest to average linear facial augmentations. What these modest implant sizes do is primarily create some angularity/convexity at the important facial bony areas as well as more pronounced connections between them
The one exception would be that of the elevation of the vertical infraorbital rim which was 6mms. A low infraorbital rim level and rounded lower eyelids require some significant rim elevation.


 Under general anesthesia and through a 2 cm submental skin incision and paired posterior vestibular incisions, the custom jawline implant as placed in a front to back insertion technique as a single implant. The custom infraorbital-malar implants were placed through lateral lower subciliary eyelid incisions.
Under general anesthesia and through a 2 cm submental skin incision and paired posterior vestibular incisions, the custom jawline implant as placed in a front to back insertion technique as a single implant. The custom infraorbital-malar implants were placed through lateral lower subciliary eyelid incisions.
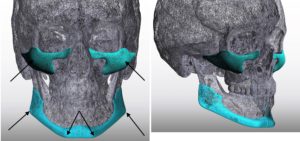 The value of many custom facial implant designs is in their coverage of larger surface bone areas in a connected fashion. While standard facial implants are often judged by their maximum projected linear increases, such an assessment for custom facial implants overlooks their more powerful effect of surface area and connectivity. Thus it often does not take as much projection at the prominence areas as one thinks to create a very visible external effect. In male facial masculinization the linear lines of the mid- and lower face are enhanced with focus on what linear measurements are desired at the ‘corners’. For some men a little bit can go a long way and this should be borne in mind with designing implants for the patient with a smaller overall face.
The value of many custom facial implant designs is in their coverage of larger surface bone areas in a connected fashion. While standard facial implants are often judged by their maximum projected linear increases, such an assessment for custom facial implants overlooks their more powerful effect of surface area and connectivity. Thus it often does not take as much projection at the prominence areas as one thinks to create a very visible external effect. In male facial masculinization the linear lines of the mid- and lower face are enhanced with focus on what linear measurements are desired at the ‘corners’. For some men a little bit can go a long way and this should be borne in mind with designing implants for the patient with a smaller overall face.
Case Highlights:
1) Softer features in a young male face is usually due to mild underdevelopment of the curved lines of the face.
2) It is no uncommon that a softer jawline is associated with equally soft cheek and under eye support as well.
3) Custom infraorbital-malar and jawline implants do not have to be big to have an effective facial masculinization effect.
Dr. Barry Eppley
Indianapolis, Indiana