

Background: The smooth shape of the skull can be disrupted by a variety of surface contour irregularities. Protrusions, indentations and ridges can occur anywhere along its bony surfaces and are most evident when the view of the scalp is not impeded by hair. With today’s male hairstyles of shaved heads being an accepted and attractive feature, any such surface irregularities become apparent and can mar an otherwise aesthetic smooth skull shape.
The skull is particularly prone to indentations or flat areas on the back of the head. This is not a surprise given the variety of forces the back of the head is esposed to both in utero and after birth. This certainly explains many occipital asymmetries and flat areas that are not uncommon. But distinct indentations or spot areas of depression are not as easily explained. If they occur in the midline they may be the result of sutural fusion areas in which incomplete bone fill has occurred.
Filling in a skull indentation requires two fundamental concepts…the material of implantation and the surgical access to place it. Ideally a truly injectable approach has the most appeal but it becomes necessary to release and lift the soft tissues off the bone to make a subperiosteal pocket that becomes confluent with the surrounding bone contour. Then there is a material that has the strength to fill the defect and support the released soft tissues and can be injected…which does not currently exist.
 Case Study: This young male with a shaved head was bothered by a distinct circular thumbprint-sized skull defect on the back of his head. By palpation it was located in the midline low on the occipital bone and just above a discernible occipital knob felt just below it.
Case Study: This young male with a shaved head was bothered by a distinct circular thumbprint-sized skull defect on the back of his head. By palpation it was located in the midline low on the occipital bone and just above a discernible occipital knob felt just below it.



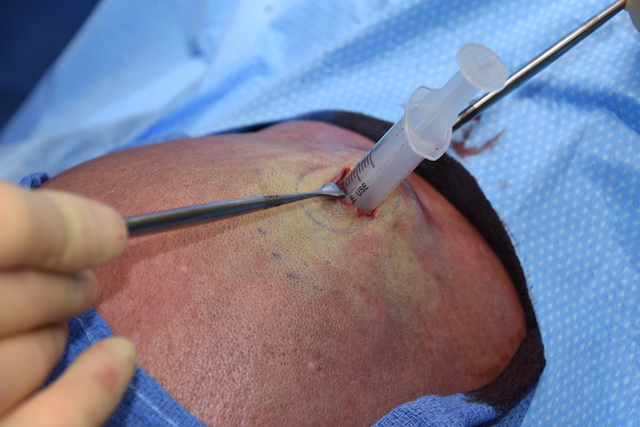
 Under general anesthesia and in the prone position a 1.5 cm horizontal scalp incision was made directly over it. Through a scalp thickness well over a cm, a subperiosteal pocket was made in a wide circular fashion up into the more normal surrounding bone. Using PMMA bone cement mixed with antibiotic powder, it was loaded into a 5cc syringe with an open end. Through the incision the barrel of the syringe was placed and the cement injected. From the outside the cement was massaged through the scalp into a smooth shape and allowed to set firm. Deep galea sutures were placed over the set cement and the skin closed with small dissolvable sutures.
Under general anesthesia and in the prone position a 1.5 cm horizontal scalp incision was made directly over it. Through a scalp thickness well over a cm, a subperiosteal pocket was made in a wide circular fashion up into the more normal surrounding bone. Using PMMA bone cement mixed with antibiotic powder, it was loaded into a 5cc syringe with an open end. Through the incision the barrel of the syringe was placed and the cement injected. From the outside the cement was massaged through the scalp into a smooth shape and allowed to set firm. Deep galea sutures were placed over the set cement and the skin closed with small dissolvable sutures.
Applying aesthetic principles to smaller skull contour problems, this ‘spot cranioplasty’ technique allows a discrete indentation to be filled and contoured through a very small skin incision. This works best for PMMA bone cement but could also be done using hydroxyapatite cement. The resultant small scalp incision will heal in a near imperceptible fashion.
Case Highlights:
1) Natural indentations of the skull can occur anywhere along its bony surfaces and are most prominent in men who shave their head.
2) Correcting small skull indentations require the aesthetic placement of an augmentation material.
3) One option of for a ‘spot cranioplasty’ is the injection of bone cement through a small scalp incision over it.
Dr. Barry Eppley
Indianapolis, Indiana