


Background: The back of the head is frequently called the occiput or occipital region of the skull. While there is anatomic truth in that statement, it is a bit overstated. The occipital bone actually only makes up the lower central area of the back of the head with its superior borders being the inverted v-pattern of he lambdoidal suture. Much of the visible back of the head is really made up of the paired parietal bones north of this suture line.
This becomes evident when a true or complete occipital bony skull deformity exists. The occipital bone sticks out like a round prominences with its visible edges along the lambdoidal suture lines. Such a prominence should be confused with more minor variants of occipital bone protrusions such as the occipital knob or excessively raised nuchal ridges. These are smaller occipital aesthetic prominences that involve exaggerated growths of natural topographic raised features of the bone.
Why the occipital bone is isolation would overgrow while the rest of the skull develops a more normal shape is not known. But regardless of the reason those patients so afflicted (usually men) find it to be an aesthetically disturbing feature.

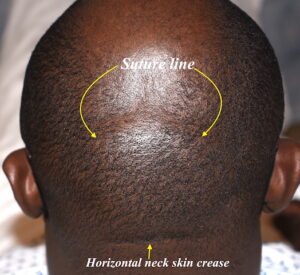 Case Study: This male has been bothered since he was a child by the protrusion on the back of his head. He did not like to go in public without wearing some head covering/cap. The prominence as a larger round projection in which the upper edge could be easily seen as the suture line.
Case Study: This male has been bothered since he was a child by the protrusion on the back of his head. He did not like to go in public without wearing some head covering/cap. The prominence as a larger round projection in which the upper edge could be easily seen as the suture line.
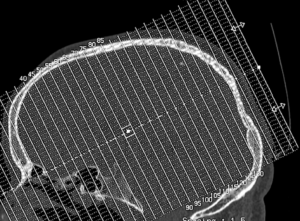
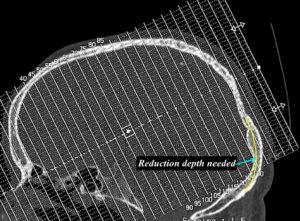 To determine that an adequate occipital bone deprojection could be safely done, a CT scan was obtained. This showed the thickness of the overly projected occipital bone and how much reduction could be done while still keeping the inner cortical table of bone intact.
To determine that an adequate occipital bone deprojection could be safely done, a CT scan was obtained. This showed the thickness of the overly projected occipital bone and how much reduction could be done while still keeping the inner cortical table of bone intact.

 Under general anesthesia and in the prone position a low incision was made in an existing horizontal neck crease. A full thickness scalp was raised where the full projection of the bone was exposed. A vertical linear cut of bone was made with a high speed drill down the middle of the bony bulge from the central lambdoid suture line to establish a good and safe bone reduction level. Similar bone channels were made in more oblique directions as well. These channels permitted a quadrant approach to be taken to the bone reduction which helps with creating a more even reduced bone contour.
Under general anesthesia and in the prone position a low incision was made in an existing horizontal neck crease. A full thickness scalp was raised where the full projection of the bone was exposed. A vertical linear cut of bone was made with a high speed drill down the middle of the bony bulge from the central lambdoid suture line to establish a good and safe bone reduction level. Similar bone channels were made in more oblique directions as well. These channels permitted a quadrant approach to be taken to the bone reduction which helps with creating a more even reduced bone contour.
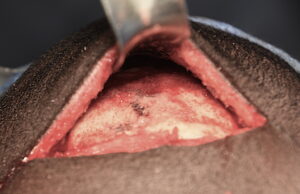 Once the bone was maximally reduced any residual bone bleeders were stopped by bone wax coverage. The bone reduction averaged 6mms with the need to keep a curved shape to the back of his head.
Once the bone was maximally reduced any residual bone bleeders were stopped by bone wax coverage. The bone reduction averaged 6mms with the need to keep a curved shape to the back of his head.

 When significant skull bone is removed it is important to recognize that excessive scalp tissue may exist. If not removed this could leave an enhanced soft tissue roll over the removed skull bone. Thus his scalp flap was pulled down and excessive scalp tissue was removed and the scalp tuck closed.
When significant skull bone is removed it is important to recognize that excessive scalp tissue may exist. If not removed this could leave an enhanced soft tissue roll over the removed skull bone. Thus his scalp flap was pulled down and excessive scalp tissue was removed and the scalp tuck closed.



 In occipital protrusion reduction, maximal bone reduction needs to be done down to the inner table of the skull with an overlying scalp tuck. This creates the opportunity for the best back of the head reshaping effect. Using an existing horizontal neck skin crease (if it exists), while making the procedure harder to perform allows the scar line to be at where a neck crease already exists.
In occipital protrusion reduction, maximal bone reduction needs to be done down to the inner table of the skull with an overlying scalp tuck. This creates the opportunity for the best back of the head reshaping effect. Using an existing horizontal neck skin crease (if it exists), while making the procedure harder to perform allows the scar line to be at where a neck crease already exists.
Case Highlights:
1) The visible occipital bone occupies a lower central position on the back of the head and, when overgrown, produces a larger round protrusion along the lambdoidal suture lines.
2) When possible occipital bone protrusion reduction should be done through a low horizontal neck skin crease.
3) Most true occipital bone reductions will require a scalp excision/tuck for the smoothest shape result.
Dr. Barry Eppley
Indianapolis, Indiana