

Background: Aesthetic deformities of the skull disrupt a pleasing convexity to its shape. These disruptions can consist of excesses and deficiencies at various skull locations. High or long skull excesses tend to occur at the top and back of the head. Deficiencies are more ubiquitous and can occur anywhere on the bony surface of the skull from the forehead to the back of the head including the sides.
Patients that present with skull asymmetries usually have a combination of both bony deficiencies and excesses. Many such skull asymmetries are caused by cranioscoliosis, a congenital condition where the skull is rotated around a vertical axis. It is most commonly recognized and called plagiocephaly. It creates the dual skull excess/deficiency shape which most severely affects the back of the head. One side of the back of the head is flat which carries forward into the parieto-temporal area eventually creating a protrusion of the forehead on that side. The opposite side of the back of the head may have an excessive protrusion as well.
But some skull asymmetries defy the classic presentation of cranioscoliosis and have shapes that have no obvious developmental origin. The patient can well describe what us abnormal about their head and a 3D CT scan can provide the anatomic basis for it.
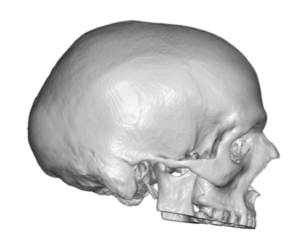
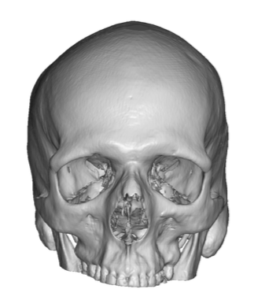 Case Study: This young male had concerns about his shape that were two fold: a central occipital protrusion and an upper occipital flattening with a right parasagittal deficiency on top. His 3D CT scan confirmed what he saw on the outside.
Case Study: This young male had concerns about his shape that were two fold: a central occipital protrusion and an upper occipital flattening with a right parasagittal deficiency on top. His 3D CT scan confirmed what he saw on the outside.
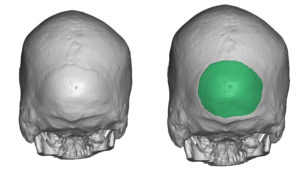
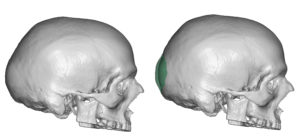
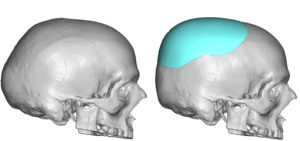
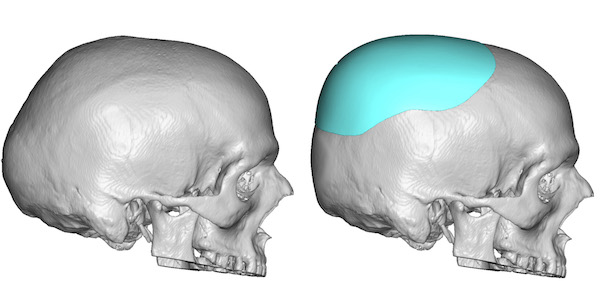
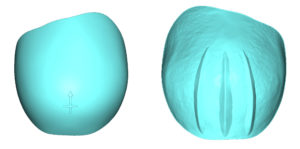
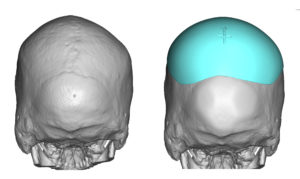 Using his 3D CT scan a surgical plan consisted of a 5mm reduction of the central occipital skull protrusion and a custom skull implant design that came up across the occiput and onto the top of the head. It was thicker and came further forward along the right parasagittal area to correct the asymmetry.
Using his 3D CT scan a surgical plan consisted of a 5mm reduction of the central occipital skull protrusion and a custom skull implant design that came up across the occiput and onto the top of the head. It was thicker and came further forward along the right parasagittal area to correct the asymmetry.


 Under general anesthesia and in the prone position a 9cm horizontal scalp incision was made at the mid-occipital scalp. Through this incision the occipital bony protrusion was reduced down to the diploic space. The scalp implant was placed superior to the reduction as per the design plan.
Under general anesthesia and in the prone position a 9cm horizontal scalp incision was made at the mid-occipital scalp. Through this incision the occipital bony protrusion was reduced down to the diploic space. The scalp implant was placed superior to the reduction as per the design plan.
 Dual modifications in aesthetic skull reshaping are not uncommon. The goal is to have a single incision by which both reduction and augmentation can be both accomplished. Because skull implants can be placed from much further distances from the incision than bone reductions can be done, the location of the protrusion determines incision placement.
Dual modifications in aesthetic skull reshaping are not uncommon. The goal is to have a single incision by which both reduction and augmentation can be both accomplished. Because skull implants can be placed from much further distances from the incision than bone reductions can be done, the location of the protrusion determines incision placement.
Case Highlights:
1) Some aesthetic skull deformities are a combination of both bony excesses and bony deficiencies.
2) In creating a better head shape bony prominences can be reduced at the same time as an augmentative custom skull implant is placed.
3) The key in combo skull reshaping is to be able to both reduction and augmentation through the same limited scalp incision.
Dr. Barry Eppley
Indianapolis, Indiana