

Background: A proportionate shape to the skull is an important element to a pleasing appearance. These heads shape proportions can be disrupted by large areas of concavities (flattening) or convexity.(protrusions) Treating skull depressions or concavities can create greater amounts of improvement through material addition which is only limited by the stretch of the overlying scalp. Skull reduction, however, are limited by what lies below it or the thickness of the skull bone itself.
The skull is composed of three well known layers, an inner and outer cortex and a marrow space (diploic space) between them. The cortical areas are much thicker than the diploic space which often is no more than 1 or 2mms thick. While the cortical thicknesses vary at different areas of the skull and by age and gender, as a general rule they are in the average range of 6 to 7mms thick.
Skull reduction is accomplished by removal of the outer cortical layer or table. Once the diploic space is exposed or nearly exposed, the safe limit of skull reduction has been achieved. An intact inner cortical layer needs to be maintained to protect the integrity of the underlying dura. While 7mms of bone removal may not seem like much, the effect is magnified by the curved surface area of reduction. But even so it must be recognized that skull reduction is a more limited procedure than that of skull augmentation.
Case Study: This young male was bothered by his occipital protrusion. It was the reason he wore his hair as long as he does.
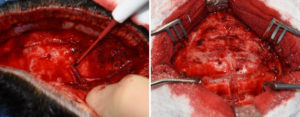
 Under general anesthesia and in the prone position a high horizontal occipital scalp incision was made and the occipital bone widely exposed. In the course of this dissection large perforating venous perforators were encountered which are not uncommon. The outer table of the skull was initially reduced by making horizontal and vertical outer table bone cuts down to the diploic space. This not only establishes the depth of the skull reduction that can be done but also creates a grid by which bone can be removed in an organized manner.
Under general anesthesia and in the prone position a high horizontal occipital scalp incision was made and the occipital bone widely exposed. In the course of this dissection large perforating venous perforators were encountered which are not uncommon. The outer table of the skull was initially reduced by making horizontal and vertical outer table bone cuts down to the diploic space. This not only establishes the depth of the skull reduction that can be done but also creates a grid by which bone can be removed in an organized manner.
 The final intraoperative result showed a modest occipital reduction but the most that can be safely removed.
The final intraoperative result showed a modest occipital reduction but the most that can be safely removed.
An important preoperative consideration is whether the amount of skull reduction that can be done can create the type of result that will make the patient satisfied. One would think that preoperative x-rays would be helpful in that regard but all they will do is show the thicknesses of the different skull layers. This 2D image does not necessarily translate into what the 3D effect of the skull reduction effect will be.
Case Highlights:
1) Skull reductions can be an effective procedure based on how much reduction is needed and the thickness of the skull bone.
2) Outer table removal of bone is what can be safely removed down to the diploic space.
3) To ensure a smooth and evenly removed bone surface a grid pattern reduction technique is used.
Dr. Barry Eppley
Indianapolis, Indiana