


Background: The sliding genioplasty is an historic autologous chin augmentation procedure that has a long history. And while it is true that the down fractured bone is moved outward it really isn’t a sliding procedure anymore and hasn’t been for over almost 40 years. Originally the cut bone segment was slid forward along the osteotomy line because the only method of fixation was wires or sutures. Thus keeping the bone in contact was unavoidable with the cinching effect of the looped fixation. In fact the slid forward movement was controlled by the distance between the front and back cortex of the chin bone which was where the wires were passed. It was not a very precise chin movement procedure.
But with the introduction of plates and screws, which can better control the position of the chin bone, multidimensonal (horizontal and vertical) chin changes are possible in a controlled fashion. While numerous chin plate fixation styles exist most are made in a step shape meaning there is a straight horizontal section of the plate which is done in a numeric horizontal progression. (2 to 28mms) While this is effective for specific horizontal movements any vertical changes must be done by bending of the plate at the screw legs.
The geometry of plate bending at the screw legs is done from the initial 90 degree angle and depends on the horizontal length of the fixation bar. There is a relationship between the horizontal length of the bar and the amount of vertical lengthening needed. The shorter the horizontal length of the plate is the greater angle (bend) is needed to create the desired vertical lengthening.
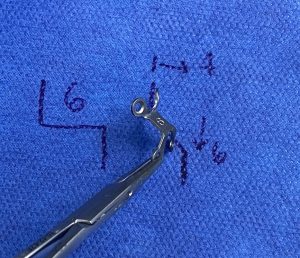 Case Study: This female desired chin augmentation by a bony genioplasty. Preoperative measurements determined that she wanted 6mms horizontal projection and 4mm vertical lengthening. To achieve this effect the plate needed to be bent at a 45 degree angle.
Case Study: This female desired chin augmentation by a bony genioplasty. Preoperative measurements determined that she wanted 6mms horizontal projection and 4mm vertical lengthening. To achieve this effect the plate needed to be bent at a 45 degree angle.
 Under general anesthesia and through an intraoral approach the chin was downfractured and the chin bone moved and the plate applied with 2 screws in the upper and lower legs.
Under general anesthesia and through an intraoral approach the chin was downfractured and the chin bone moved and the plate applied with 2 screws in the upper and lower legs.

 The intraoperative change reflected the near 45 degree change in chin projection.
The intraoperative change reflected the near 45 degree change in chin projection.
Even in a pure horizontal chin movement there is an opening along the line of the osteotomy cut. This its because the osteotomy cut is angled no matter how low and posteriorly the cut is made. If the chin bone stayed exactly along the osteotomy cut the chin would actually be vertically shortened. When deliberate vertical lengthening is needed along with horizontal projection the chin osteotomy becomes an opening wedge.
Case Highlights:
1) Many genioplasties today are not sliding in the historic sense but two-dimensional chin augmentative changes.
2) Plate fixation makes multidimensional chin changes possible through plate bending.
3) The required bending of the step plate in multidimensional chin changes is done through angular geometry.
Dr. Barry Eppley
World-Renowned Plastic Surgeon