

Background: In larger skull implant augmentations it is necessary to undergo a 1st stage scalp expansion. What defines a skull implant size that requires an initial scalp expansion depends on several factors, the most important of which is the scalp’s ability to stretch to accommodate the size of the implant underneath it. There is not an exact science to it but assessing the thickness of the scalp and how flexible (stretchy) it may be is based on skin pigmentation and hair color as well as the patient’’s body type. The greater the skin pigment the darker the hair the thicker the scalp will be. Increased scalp thickness equals greater flexibility. Thicker larger body frames also have increased scalp thicknesses.
With placement of the scalp tissue expander little to no volume is initially placed. Self inflations are started within one to two weeks after placement and continue twice a week at 10cc injected volume. With most scalp inflations around or over 200cc, it takes 3 to 4 months to achieve the desired effect before surgery. Ideally the inflation volume should equal or even be greater than the volume of designed skull implant.
Second stage placement of the custom skull implant requires an obvious tissue expander removal. What is not obvious is that besides the expander removal the capsule must be removed from the underlying bone surface (subtotal capsuletomies) as well as expanding the existing expander pocket. (circumferential capsulotomies) to allow the skull implant to fit. This is no easy task and is far more challenging than placing the tissue expander. To place the skull implant it will usually be designed in several pieces (2 to 4) to allow it to fit through a small scalp incision. It is then reassembled once inside the pocket like puzzles pieces…which is also a challenge of its own.
Case Study: This female desired to have a significant skull augmentation with a thin tight scalp. She had two prior hair transplantations which is a primary indicator for the need for a 1st stage scalp expansion.
 A 15cm diameter round scalp tissue expander with a distal port was initially placed through her strip harvest hair transplant scars on the back of her head. No volume was initially placed into it.
A 15cm diameter round scalp tissue expander with a distal port was initially placed through her strip harvest hair transplant scars on the back of her head. No volume was initially placed into it.
Because of her tight scalp and prior strip harvests she gradually inflated the tissue expander to 200ccs volume over a six month time period.
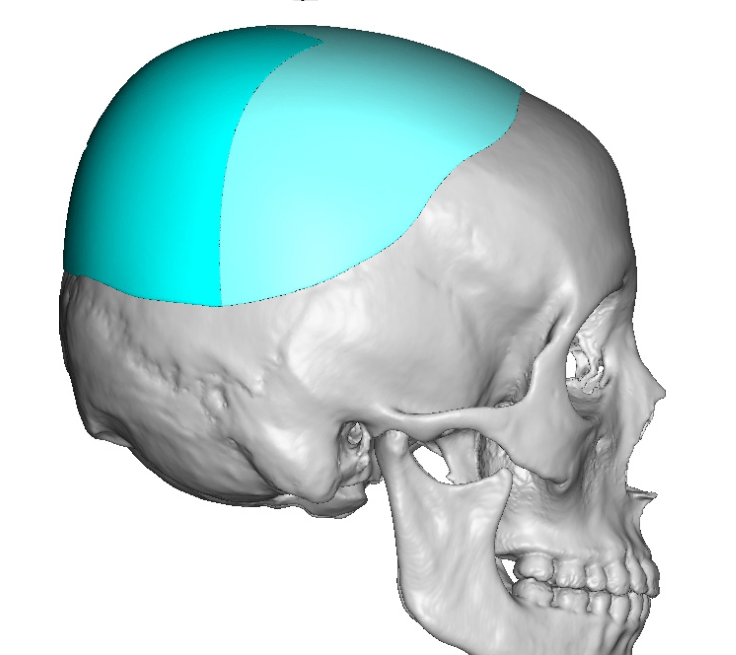
 In the interim a custom skull implant was designed for her desired area of head augmentation. The implant volume was 170ccs. It was designed as a two-piece implant with a horizontal split with a geometric interface.
In the interim a custom skull implant was designed for her desired area of head augmentation. The implant volume was 170ccs. It was designed as a two-piece implant with a horizontal split with a geometric interface.
 Six months later due to the need for a very slow inflation period and other issues she returned for the custom skull implant placement. Through the same length scalp incision on the back of her head, the tissue expander and its remote port were removed. The capsule over the entire bine surface where the expander was sitting was removed. As the skull implant’s footprint was bigger than that of the tissue expander the pocket was expanded in all direction through releasing capsulotomies.
Six months later due to the need for a very slow inflation period and other issues she returned for the custom skull implant placement. Through the same length scalp incision on the back of her head, the tissue expander and its remote port were removed. The capsule over the entire bine surface where the expander was sitting was removed. As the skull implant’s footprint was bigger than that of the tissue expander the pocket was expanded in all direction through releasing capsulotomies.

 Once an adequate pocket was developed the custom skull implant was passed through the incision in two pieces. The front end went first and back end second. By external feel the two implants pieced were put together. Because the seam of the two implant pieces was anterior to the incision a slit was made in the posterior implant segment at the incision level through which sutures were passed between the two implant segments to pull them together tight at its unseen seam.
Once an adequate pocket was developed the custom skull implant was passed through the incision in two pieces. The front end went first and back end second. By external feel the two implants pieced were put together. Because the seam of the two implant pieces was anterior to the incision a slit was made in the posterior implant segment at the incision level through which sutures were passed between the two implant segments to pull them together tight at its unseen seam.
The scalp incision was closed over a drain. The drain was removed 4 days later. She went on to heal uneventfully with the maximum amount of skull augmentation that could be achieved in her naturally thin scalp that has been further compromised by prior strip harvest hair transplantations.
Case Highlights:
1) Thin Caucasian females who desire larger skull augmentations will always require a two stage approach to it.
2) After the initial scalp tissue expander placement inflations should be slowly placed and ultimately must equal or exceed the volume of the designed skull implant.
3) Larger skull implants are designed and placed in multiple pieces with geometric interfaces to keep the scalp incision as small as possible.
Dr. Barry Eppley
World-Renowned Plastic Surgeon