


Plagiocephaly is one of the recognized and perhaps most common of all the congenital skull deformities. By its name it means an oblique or twisted skull shape where the skull appears rotated around its central axis affecting the back, sides and forehead giving them an asymmetric shape. It typically affects the back of the head more than the face in most cases.
Because the origins of plagiocephaly are not associated with any specific cranial suture line (not a true craniosynostosis) it is not a skull condition that is typically treated by surgery at an early age. Most plagiocephalies are treated by non-surgical helmet therapy, some more successfully than others.
Most of the time the plagiocephaly may be improved by early helmet therapy but often the condition is not recognized until after the time period of when helmet therapy would be most effective. One commonly held belief about many plagiocephalies is that the patient will outgrow it with time…meaning that the growth of the brain will push the skull back into a better shape. But this rarely occurs. Some improvement may occur but the asymmetric shape of the hard remains.
As a result there are many adult patients with varying degrees of plagiocephaly that walk around untreated. Many are of a minor degree and are not bothered by it and the head’s shape may be well camouflaged with hair. But there others who are extremely bothered by it and I often hear of their methods of camouflage such as hats and hairstyles.
The basic concepts in the treatment of adult plagiocephaly are the skull reshaping options of bone reduction (for protrusions) and bone augmentation. (for deficiencies) To understand these approaches let’s look at a recent plagiocephaly case that I treated who employed every available treatment option.

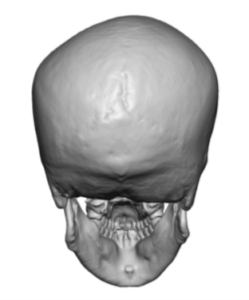
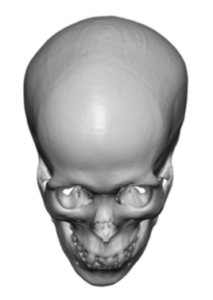 In his preoperative 3D CT skull CT scan it demonstrates a right-sided plagiocephalic head shape…which means the twist is to the right. (right sided plagiocephaly is the most common) This creates a right back of head flattening, some left temporo-parietal protrusion, right forehead protrusion, and left forehead ‘recession’. The position of the ear holes (external auditory canals) are also asymmetric along with the attached external ears with the right being further forward than that of the left.
In his preoperative 3D CT skull CT scan it demonstrates a right-sided plagiocephalic head shape…which means the twist is to the right. (right sided plagiocephaly is the most common) This creates a right back of head flattening, some left temporo-parietal protrusion, right forehead protrusion, and left forehead ‘recession’. The position of the ear holes (external auditory canals) are also asymmetric along with the attached external ears with the right being further forward than that of the left.
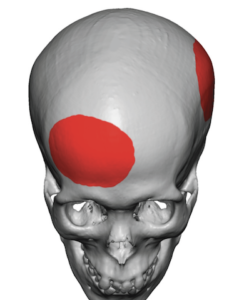
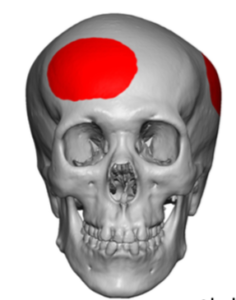 Options for skull bone reduction include the right forehead and the left temporo-parietal areas. Such protrusion reductions are limited to the 4 to 5mm range given the thickness of the bone.
Options for skull bone reduction include the right forehead and the left temporo-parietal areas. Such protrusion reductions are limited to the 4 to 5mm range given the thickness of the bone.
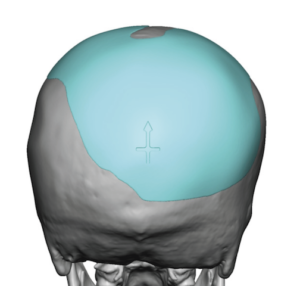
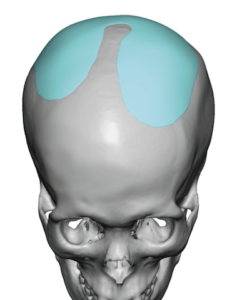
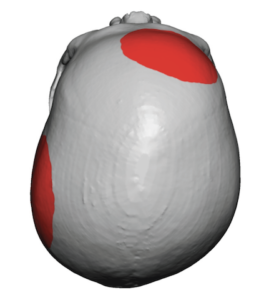
 Options for skull augmentation are more significant with larger surface area coverages. These include the back of the head and any parasagittal regions on the top of the head that may also be affected.
Options for skull augmentation are more significant with larger surface area coverages. These include the back of the head and any parasagittal regions on the top of the head that may also be affected.
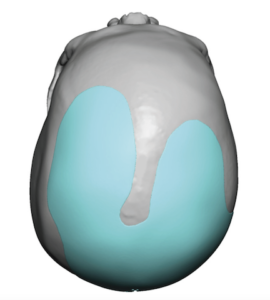
In most cases of adult plagiocephaly that I see augmentation of the flat back of the head is the #1 priority and provides the most significant improvement. Custom skull implant designs provide the most accurate method to both identify and cover the deficient skull areas. In some cases the prominent forehead side is requested to be reduced but this has to take into consideration the location of the incision and resultant scar to do so. Setback of the protruding ear on the anteriorly rotated side is commonly done and is the simplest of the sequelae of plagiocephaly issues to correct.
Dr. Barry Eppley
Indianapolis, Indiana