

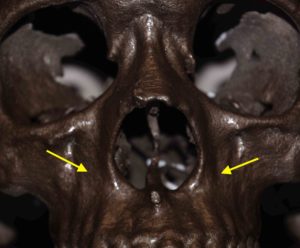
 A concave central midface that lacks projection creates a less than desirable appearance that can give the face a more aged appearance. Flatter midfaces are almost always associated with deeper nasolabial fold area or a premature development of them. Paranasal implants are a proven method to augment the natural concave bony areas around the pyriform apertures. Bony augmentation underneath the nostrils out to the canine fossa not only adds projection to the central midface but it also decreases the depth of the nasolabial folds by the side of the nose. (increases the nasolabial angle) It may also provide some increased nasal tip projection in certain patients. Such changes are associated with a more youthful and improved facial profile.
A concave central midface that lacks projection creates a less than desirable appearance that can give the face a more aged appearance. Flatter midfaces are almost always associated with deeper nasolabial fold area or a premature development of them. Paranasal implants are a proven method to augment the natural concave bony areas around the pyriform apertures. Bony augmentation underneath the nostrils out to the canine fossa not only adds projection to the central midface but it also decreases the depth of the nasolabial folds by the side of the nose. (increases the nasolabial angle) It may also provide some increased nasal tip projection in certain patients. Such changes are associated with a more youthful and improved facial profile.
Preoperative computer imaging is usually considered essential to ensure that the patient’s mid facial augmentation goals, what the patient’s anatomy and the what the dimensions of the implant will achieve are similar. Such imaging is also important to determine how much projection is desired. The ePTFE paranasal implant comes in two thicknesses (5 and 6mms) which can be reduced by intraoperative carving with a scalpel is needed.
In some patients postsurgical alar base widening may occur after paranasal augmentation may be an adverse effect in those patients with midfacial and paranasal volume deficits. As a result paranasal augmentation may need to be coupled with alar reduction to ensure an improved central midfacial/nasal appearance.
The procedure can be performed under local, IV sedation or general anesthesia depending upon if it is an isolated procedure or as part of other facials surgeries. After intraoral infiltration with a 1% Lidocaine and 1:100,000 epinephrine solution for hemostasis, bilateral high vestibular incisions under the upper lip and lateral to the pyriform aperture are made that do not connect. It is important that these incisions are well above the gingivobuccal sulcus tis ensure that an adequate inferior musculomucosal cuff of tissue persists for a competent wound closure. Wide subperiosteal dissection is done ensuring that the medial dissection does not violate the nasal mucosa at the pyriform aperture. Dissection is also carried around the pyriform aperture medial to but not crossing the anterior nasal spine.
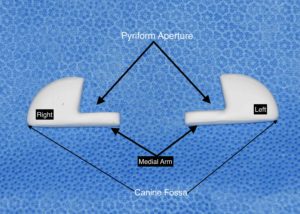 Made of solid ePTFE, these new paranasal implants are a crescent shaped left-right pair and available in small, medium and large sizes in two different thicknesses. In selecting implant size thickness and surface area coverage are the two considerations. It is helpful to have intraoperative sizers available to help with that decision. But the two rules to follow in paranasal augmentation is: 1) at least 5mms thickness is needed by most patients, and 2) the footprint of the implant should extend lateral enough to cover the canine fossa to avoid a bump-like external appearance.
Made of solid ePTFE, these new paranasal implants are a crescent shaped left-right pair and available in small, medium and large sizes in two different thicknesses. In selecting implant size thickness and surface area coverage are the two considerations. It is helpful to have intraoperative sizers available to help with that decision. But the two rules to follow in paranasal augmentation is: 1) at least 5mms thickness is needed by most patients, and 2) the footprint of the implant should extend lateral enough to cover the canine fossa to avoid a bump-like external appearance.
ePTFE paranasal implants are easily customizable with a scalpel (#10 or #15 blade) to modify their thickness, edges or extent of the medial arms or main body of their footprint. Pay particular attention to the contour of the implant laterally over the canine fossa to ensure that a smooth transition exists and an external palpable edge is not felt.
Fixation of the implant can be done with sutures, screws or by placing perfusion holes through the implant for tissue ingrowth. Typically the limits of the pocket dissection and the tightness of the implant fit into it does not make firm fixation essential. If screws fixation is to bee used a self-tapping 8mm screw is sufficient, one per side. The technique I prefer most of the time today is that or perfusion holes where tissue ingrowth occurs and is ultimately what secures them in place. Twi perfusion holes per side is what is used of 4mm diameters. After irrigating out with an antibacterial solution a two layer musculomucosal closure is done over the implant.
ePTFE paranasal implants have numerous advantages over the older peripyriform silicone implants. They have a better shape and can be easily contoured to fit the patient. That also allows for some tissue adherence to them although this does not take their removal unduly difficult like other tissue adherent materials.
Dr. Barry Eppley
Indianapolis, Indiana