

Ear reconstruction of congenital or traumatic injuries often involves the need for multiple tissue layers to rebuild the ear. A cartilage framework and a vascularized layer on top of the cartilage onto which a skin graft is placed on its outer surface is essential in many major full thickness ear absences or losses. In creating the framework for whatever part of the ear is missing it is important to remember that only the raised or convex surfaces of the ear need a framework. All concave contours of the ear can be unsupported and allowed to collapse in between the convex framework segments.
 Rib cartilage remains the workhorse framework material in ear reconstruction. Besides having an ample supply to harvest and use, the longer rib segments from the cartilaginous subcostal area are well suited to be shaped and bent into a curved shape like that of the helical rim. Whether a short segment like the end of rib #10 or then longer ribs #8 and #9 depends on how much helical rim is needed. In the most extensive form of ear reconstruction in congenital microtia, portions of ribs #6,7, 8 and 9 are used.
Rib cartilage remains the workhorse framework material in ear reconstruction. Besides having an ample supply to harvest and use, the longer rib segments from the cartilaginous subcostal area are well suited to be shaped and bent into a curved shape like that of the helical rim. Whether a short segment like the end of rib #10 or then longer ribs #8 and #9 depends on how much helical rim is needed. In the most extensive form of ear reconstruction in congenital microtia, portions of ribs #6,7, 8 and 9 are used.
While the subcostal rib lengths are adequate they must be thinned and bent into an arc-like shape. The ability to do so depends on the natural elasticity of the cartilage. In children and teens this is never a problem but can be so in adults particularly older adults. As one ages the ribs develop variable amounts of calcification and become stiffer. When thinned and bent they become more brittle and prone to fracture.
A technique I have found useful in adult rib shaping for ears is to use a metal template to support a long bend into an arc shape. Specifically a 1.5mm thin titanium fixation plate can be used. The desired bend is first made in the metal plate to which the rib cartilage is then attached by permanent sutures with the knots on the inside. There even a brittle rib in an older adult can get the desired shape that is stable.

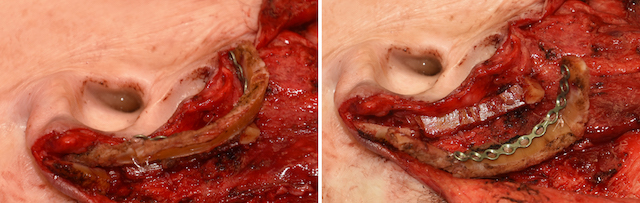
 This case example of an ear reconstruction illustrates this rib shaping technique. Having lost most of the outer helix due to a burn injury, reconstruction was planned for a rib graft covered by a temporoparietal fascial flap and a split thickness skin graft. In harvesting the cartilaginous portion of rib #10 its end fractured off. The longer rib #9 was then harvested. In thinning it and creating the helical shape it fractured in two areas. A long 1.5mms titanium plate was then used to attach the the rib #9 segments. Rib #10 was then used as a platform to support the helical rim rib graft reconstruction.
This case example of an ear reconstruction illustrates this rib shaping technique. Having lost most of the outer helix due to a burn injury, reconstruction was planned for a rib graft covered by a temporoparietal fascial flap and a split thickness skin graft. In harvesting the cartilaginous portion of rib #10 its end fractured off. The longer rib #9 was then harvested. In thinning it and creating the helical shape it fractured in two areas. A long 1.5mms titanium plate was then used to attach the the rib #9 segments. Rib #10 was then used as a platform to support the helical rim rib graft reconstruction.
Dr. Barry Eppley
Indianapolis, Indiana