

Background: The most common aesthetic skull deformity is that of the flat back of the head. This occurs most commonly from in utero or postnatal infant positioning and also has a strong genetic tendency amongst certain ethnic groups. (e.g., Asian) While a flat back of the head has no detrimental intracranial or neurologic effects, it can be very psychologically bothersome to some people. To those so affected, it causes a variety of efforts at hairstyle and hat management to camouflage the shape of the skull.
A variety of augmentation procedures have been done over the years for the flat back of the head deformity. It is merely a question of what materials have been used, how they are shaped and what type of incisional access is needed to do so. Injectable materials like synthetic fillers and fat, while appealing, simply do not work. The scalp is not like the face, breasts or buttocks. It is much stiffer and has no real fatty layer into which filler materials be easily placed. While some injected fat may survive, it runs a high risk of being irregular and can never create much overall volume augmentation.
Bone cements have been the most popular skull augmentation materials. While they can be effective they require fairly long scalp incisions to properly place and shape them. When placing them through smaller incisions they run the risk of palpable irregularities and edge transitions. The kocation of the incision is often needed right near or over the cement application which potentially poses a healing issue when the scalp closure is very tight.
In my practice, bone cements have largely given way to custom skull implants made from the patient’s 3D CT scan. This method offers significant advantages including a precise shape and thickness augmentation, a much lower risk of edge transition and irregularities, shorter operative times and a scalp incision that is located away from the implant’s maximal tension of the overlying scalp
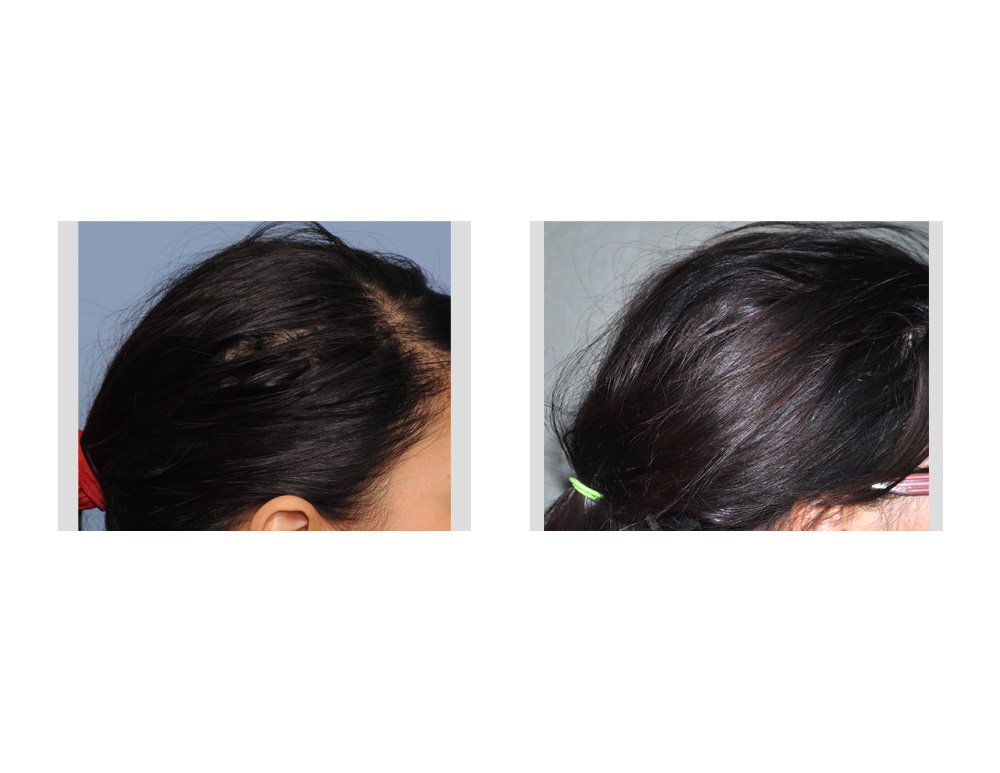
Case Study: This 30 year-old female had long been bothered by the flatness at the top of her head. She styled her hair to puff it up in the back to add volume to the back of her head. She finally wanted a more definitive and permanent solution. She did have a very pertinent prior cosmetic surgery history having had a strip graft harvest from the back of her head for hair transplantation to lower her frontal hairline.
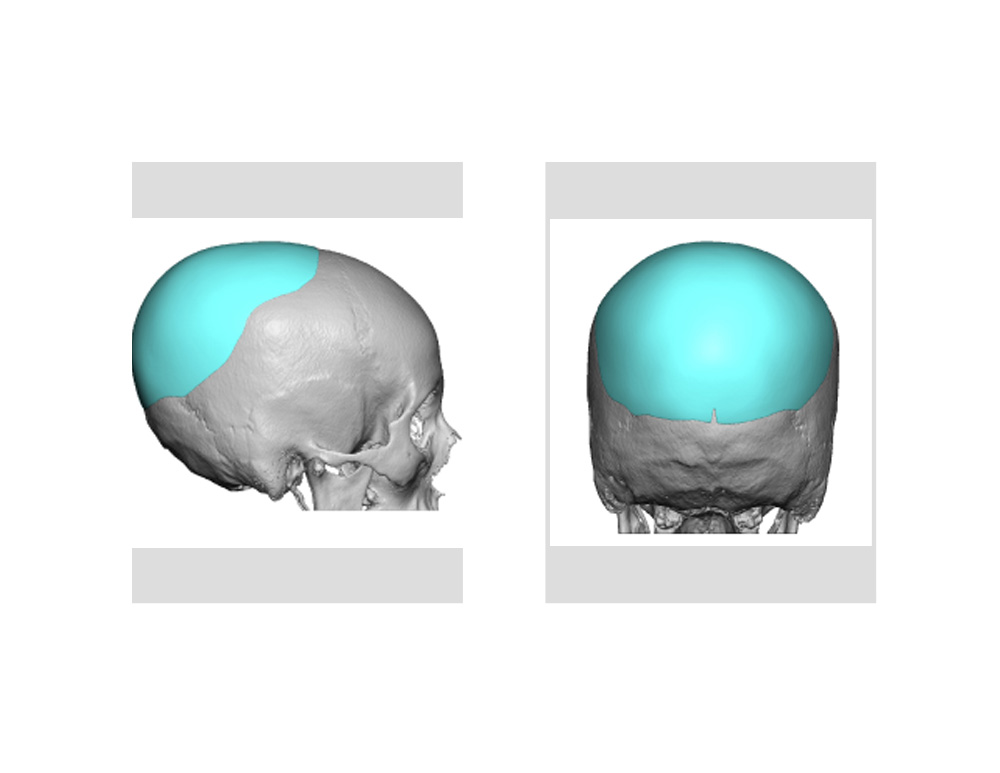
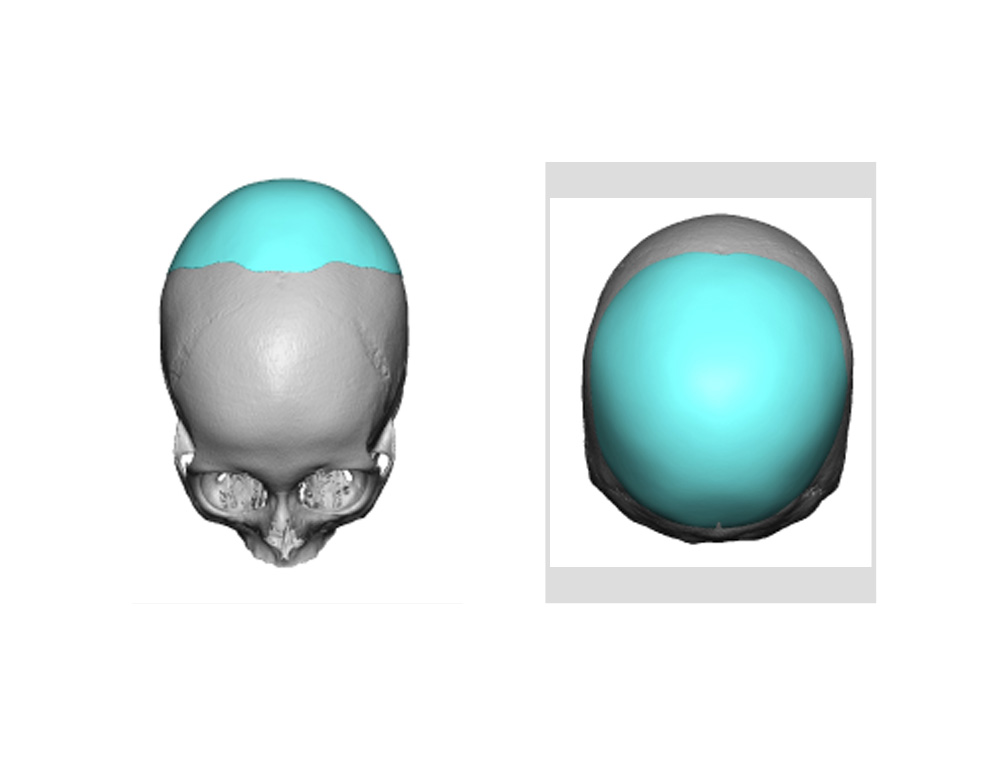 A 3D CT scan was used to design a silicone occipital implant to cover the back of her head. Its maximal thickness was 12mm in the central projection area. Because of her prior hair transplant, she had lost at least 1 cm of scalp flexibility. The thickness of the implant was kept to 12mm to ensure that it would fit without undue tension on the scalp incision and also not to compromise the blood flow to the central scalp over the implant.
A 3D CT scan was used to design a silicone occipital implant to cover the back of her head. Its maximal thickness was 12mm in the central projection area. Because of her prior hair transplant, she had lost at least 1 cm of scalp flexibility. The thickness of the implant was kept to 12mm to ensure that it would fit without undue tension on the scalp incision and also not to compromise the blood flow to the central scalp over the implant.
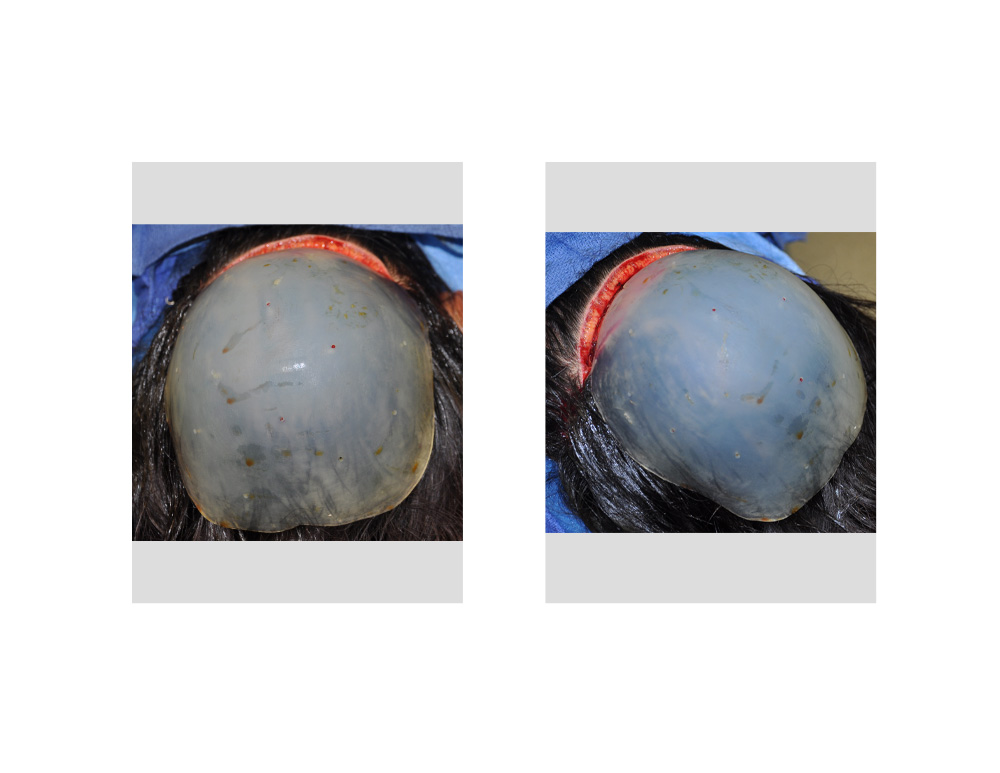
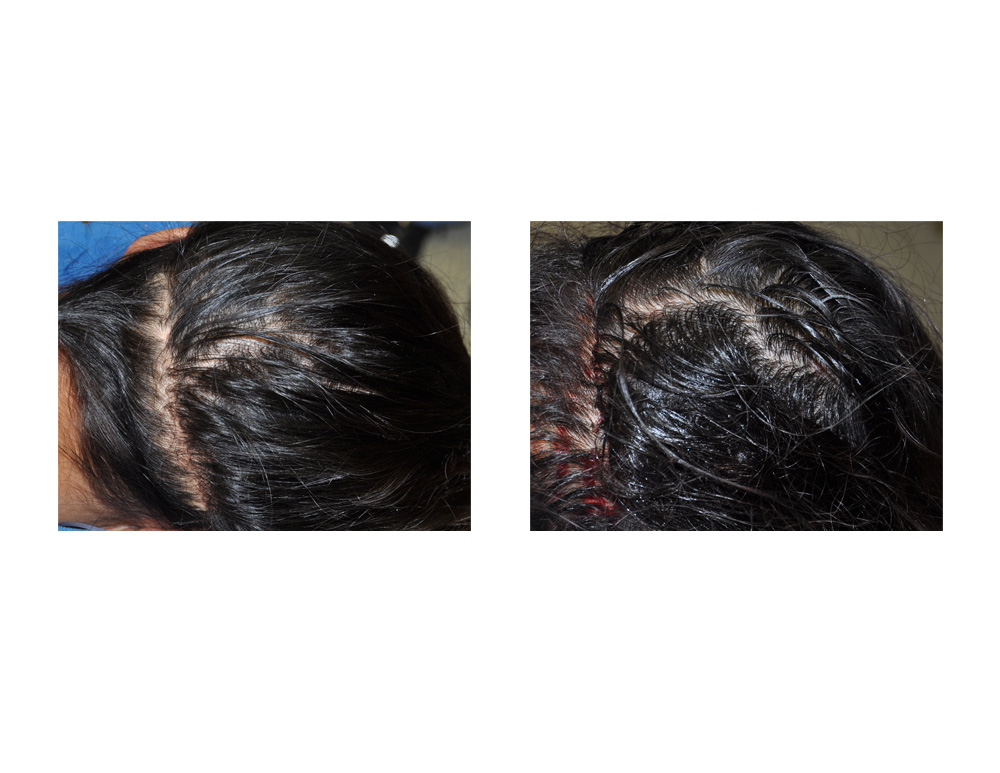 Under general anesthesia and in the prone position, her prior hair transplant scar was used for access. At the tail end of the incisions the occipital neurovascular bundles were identified and preserved. Long curved instruments were used to develop a subperiosteal pocket around the curved contours of the back of the skull. The custom implant was prepared by placing multiple perfusion holes using a 2mm punch. It was fairly easily inserted, positioned and the scalp incision closed with some tension.
Under general anesthesia and in the prone position, her prior hair transplant scar was used for access. At the tail end of the incisions the occipital neurovascular bundles were identified and preserved. Long curved instruments were used to develop a subperiosteal pocket around the curved contours of the back of the skull. The custom implant was prepared by placing multiple perfusion holes using a 2mm punch. It was fairly easily inserted, positioned and the scalp incision closed with some tension.
 A custom skull implant for a flat back of the head offers the most predictable outcome with the lowest risk of complications or need for revisional surgery in my experience. Designing the implant shape and thickness that the scalp can tolerate is the ‘art’ in the process and that will differ somewhat for each patient. Some patients will find that the amount of augmentation may be less than they desire as a single stage procedure. If one desires much larger amounts of occipital augmentation, a two-stage approach can be done with a first stage scalp tissue expander.
A custom skull implant for a flat back of the head offers the most predictable outcome with the lowest risk of complications or need for revisional surgery in my experience. Designing the implant shape and thickness that the scalp can tolerate is the ‘art’ in the process and that will differ somewhat for each patient. Some patients will find that the amount of augmentation may be less than they desire as a single stage procedure. If one desires much larger amounts of occipital augmentation, a two-stage approach can be done with a first stage scalp tissue expander.
Case Highlights:
1) Custom designed silicone implants are the most effective method for augmentation of the flat back of the head.
2) The size and thickness of a custom occipital implant is controlled by the incisional access and how much the scalp will stretch to accommodate the thickness of the implant
3) It has been my experience that 12mm to 15mms is as much implant thickness that can be placed on the back of the head.
Dr. Barry Eppley
Indianapolis, Indiana