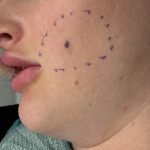
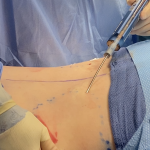
Reshaping the Round Face – Implant and Soft Tissue Reduction Strategies
For a round face, the goal is to shift from a circular, width-dominant shape to something more vertically defined and angular. With custom implants, you’re adding structure—but in round faces, soft tissue thickness is often the limiting factor, so reduction plays a bigger role than usual. Here’s how to think about the best combinations: Core Read More…