Custom Head Widening Implants Case Study
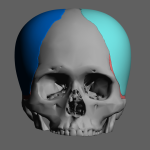
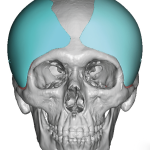
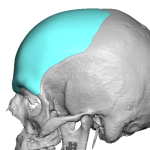
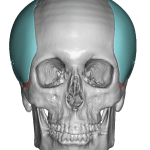
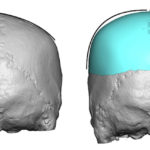
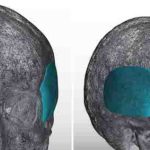
Introduction Custom head-widening implants are a highly specialized procedure performed by only a few surgeons worldwide. These implants are 3D-designed, medical-grade solid silicone devices placed along the sides of the skull—specifically over the temporal muscle region—to increase the absolute width of the head. Designed from a patient’s 3D CT scan, they typically provide 0.5–1.0 cm Read More…