Shaving of Ribcage Protrusions – Concept and Case Example
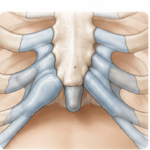
What Does Rib Shaving Mean? Shaving of ribcage protrusions is a surgical contouring procedure in which a prominent portion of a rib or ribs is reduced through excision of its outer convexity through bone or cartilage removal rather than removing the entire rib segment. Typically this is done for protrusions of the costal or cartilage-comprised Read More…