

Background: The size of the thigh (upper leg) is heavily influenced by the bulk provided by its muscle mass. Between the large femur bone and the many muscles that encircle it the thigh is always bigger than its lower leg counterpart in both length and circumference. As the connector between the pelvis and the knee the thigh’s large muscle masses responsible for a lot of the leg’s range of motion and movement.
Typically the two thighs are relatively equal in size. But there are some conditions that create thigh asymmetry due to a change in its muscle mass. Fractures and immobilization is the most common cause but that is usually a recoverable situation. Congenital births defects and tumors are the other causes. Tumor resections and radiation when one is young and developing can create a major difference in the soft tissue mass of the thigh that is permanent.
Augmentation or reconstruction of soft tissue discrepancies in the size of the thighs is a difficult challenge. The sheer amount of soft tissue that is needed leaves limited donor options from the rest of the body. Smaller defects of the thigh can be treated by fat injections if one has adequate donor sites. But larger defects are not so easily treated and the volume of inject ate needed usually far exceeds what the patient’s donor sites have to offer.
Case Study: This young middle-aged female presented with significant left thigh asymmetry as a result of a malignant tumor resection as a teenager for which she did not receive radiation. An allogeneic bone graft failed and she ultimately had a knee fusion for leg stabilization. As a result she had muscle atrophy of the thigh and calf with a difference in the overall size of the legs. She was very thin so no form of an autogenous reconstruction could be done. Measurements were made of the extent of the thigh defect from which a silicone elastomer moulage was made for silicone implant fabrication.
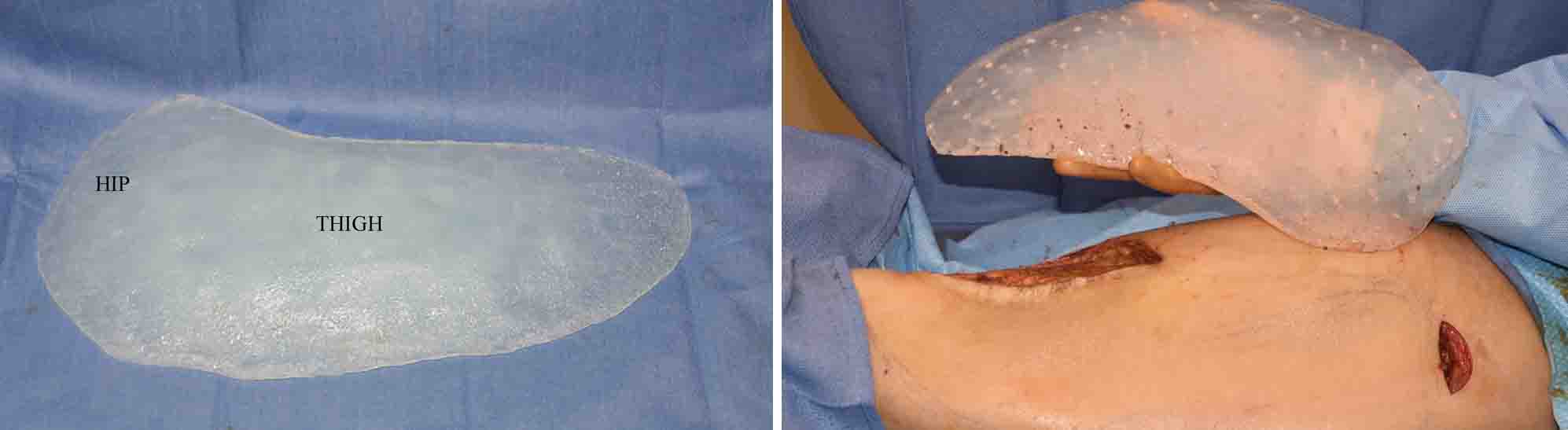
 Under general anesthesia and initially in the prone position, calf implants were placed from two popliteal fossa skin incisions for the medial and lateral gastrocnemius muscle bellies in subfascial pockets. In the supine position a one-piece hip and thigh implant was placed on top of the thigh muscle fascia from just above the knee on the anterolateral side up into the hip through an existing vertical scar in the lower half of the thigh. (combined with a small horizontal skin incision in the hip to ensure superior implant positioning. The thigh implant had multiple 4mm perfusion holes placed in it to allow for some tissue ingrowth long-term.
Under general anesthesia and initially in the prone position, calf implants were placed from two popliteal fossa skin incisions for the medial and lateral gastrocnemius muscle bellies in subfascial pockets. In the supine position a one-piece hip and thigh implant was placed on top of the thigh muscle fascia from just above the knee on the anterolateral side up into the hip through an existing vertical scar in the lower half of the thigh. (combined with a small horizontal skin incision in the hip to ensure superior implant positioning. The thigh implant had multiple 4mm perfusion holes placed in it to allow for some tissue ingrowth long-term.
Implants an option for thigh soft tissue defects resulting from muscle atrophy that is not the result of radiation effects. The material needs to be very soft and flexible to not limit movement. While smaller implants can be placed in a subfascial position, larger thigh implants will need to be placed above the fascia.
Highlights:
1) Large soft tissue asymmetries of the thigh pose significant augmentation challenges.
2) A large custom made silicone thigh implant can be designed from measurements and a moulage design.
3) Placement of a custom thigh implant is done on top of the fascia which in his case was done through a mid-thigh incision.
Dr. Barry Eppley
Indianapolis, Indiana